Download
1 / 1
10 likes | 285 Views

E N D
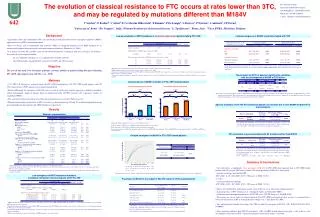
The evolution of classical resistance to FTC occurs at rates lower than 3TC, and may be regulated by mutations different than M184VV Svicher1, F Forbici2, C Alteri1, F Ceccherini Silberstein1, E Boumis2, P De Longis2, L Stuyver3, P Narciso2, A Antinori2, CF Perno21University of Rome “Tor Vergata” , Italy; 2National Institute for Infectious Diseases "L. Spallanzani", Rome, Italy; 3Virco BVBA, Mechelen, Belgium. Dr. Valentina Svicher University of Rome Tor Vergata Via Montpellier 1, Rome 00133, Italy Phone No: +39-06-72596553 e-mail: valentina.svicher@uniroma2.it 642 Low accumulation of NRTI mutations in treatment-experienced patients failing FTC+TDF Limited emergence of M184V in patients treated with TDF The analysis was performed on 1337 patients. Predictor variables considered are: sex, age, viremia and CD4 cell count at baseline , therapy length, previously and currently received drugs (including NRTI, NNRTI and PI). Only significant predictors are reported in the table a The analysis was performed in the subset of patients with sequences available both at baseline and at failure. b NRTI-resistance mutations considered are those reported in Johnson et al., 2008. c Statistically significant difference between FTC+TDF treated patients and 3TC+TDF treated patients was assessed by Fisher exact test for categorical data and by Wilcoxon test for continuous variables. d Statistically significant differences among the 3 groups of patients were assessed by Chi Squared for trend for categorical data and by Kruskal Wallis test for continuous variables. The presence of I202V at baseline significantly correlates with the development of M184V at FTC failure Low prevalence of M184V mutation in FTC+TDF-treated patients A. Patients failing first line regimen B. Treatment-experienced patients P<0.001 P<0.001 The analysis was performed in the subset of FTC+TDF treated patients with sequences available both at baseline and at failure. All RT mutations present at baseline were analyzed. The same analysis has been performed in 3TC-treated patients. In this subset of patients, no polymorphisms present at baseline resulted significantly associated with the on-treatment development of M184V. P=0.14 P=0.02 P=0.017 P=0.001 543 (71.9%) 132 (59.4%) 84 (51.0%) Specific mutations in the HIV RT connection domain can increase the in vitro M184V-mediated FTC fold resistance 61 (45.9%) % of patients with M184V Results 7 (25.9%) 4 (11.4%) Patients’ characteristics Treatment with b c P value P value FTC+TDF 3TC+TDF 3TC (naive to TDF) a Number of patients 168 249 920 Date started treatment 2006 (2005-2006) 2004 (2003-2005) 2002 (2001-2003) a The analysis was performed on 111 clones from 19 patients; the values of FTC fold resistance are derived from the real phenotypic data measured by Virco’s Antivirogram assay. The values of 3TC fold resistance were not available for the analysis. • Statistically significant differences were assessed by Fisher exact test. • The prevalence of M184V was calculated in patients failing their first line regimen. • The prevalence of M184V was calculated in treatment-experienced patients. • The overall prevalence of M184V in all patients analyzed is 38.7% in FTC+TDF-treated patients, 55.8% in 3TC+TDF-treated patients, and 68.0% in 3TC-treated/TDF not treated patients. Male, N (%) 120 (72.3) 181 (73.0) 654 (71.1) 0.91 0.88 HIV exposure, N (%) MSM 23 (19.5) 34 (18.1) 89 (18.9) 0.76 0.95 Heterosexual 35 (29.7) 59 (31.4) 138 (29.4) 0.8 0.88 IDU 52 (44.1) 89 (47.3) 239 (50.9) 0.64 0.37 Age (years), Median (IQR) 43 (38-47) 42 (38-46) 40 (36-45) 0.74 <0.001 FTC resistance may be associated with RT mutations other than M184V Viremia (log copies/ml), Median (IQR) Delayed emergence of M184V in FTC+TDF-treated patients Baseline 4.7 (3.4-5.4) 4.5 (3.3-5.1) 4.4 (3.4-5.1) 0.35 0.53 Change from baseline to failure [-3.9 [-5.2;2.5] [-3.5 [-4.8;3.7] [-3.9 [-3.3;4.9] 0.2 0.45 CD4 cell count (cells/ul), Median (IQR) Baseline 229 (127-449) 281 (170-449) 271 (135-465) 0.13 0.33 Change from baseline to failure 17 [-41.7;101.5] 7 [-76.5;133.2] 25[-41;123] 0.66 0.15 Number (%) of patients at first line regimen 35 (20.8) 27 (10.8) 165 (17.9) Coadministered drugs, N (%) NNRTI 11 (31.4) 13 (48.1) 59 (35.8) 0.18 0.37 a Sequences were collected from the Stanford HIV Drug Resistance Database; the values for increases in resistance (n-fold) are derived from the real phenotypic data measured by Virco’s Antivirogram assay. Sequences with K43E do not contain other major NRTI resistance mutations. Novel mutations associated with 3TC resistance were not identified PI 22 (62.9) 11 (40.7) 80 (48.5) 0.12 0.18 3TC+TDF Probability to develop M184V Number (%) of treatment-experienced patients 133 (79.2) 222 (89.2) 755 (82.1) FTC+TDF Coadministered drugs, N (%) NNRTI 35 (26.3) 81 (36.5) 300 (39.7) 0.06 0.01 PI 96 (72.2) 108 (48.6) 366 (48.5) <0.001 <0.001 Number of previously received drugs, Median (IQR) NRTI 4 (2-5) 4 (2-5) 3 (2-4) 0.96 <0.001 NNRTI 1 (0-1) 1 (0-1) 0 (0-1) 0.37 <0.001 Summary & Conclusions a All the 920 patients started 3TC treatment after 2000. No patients received 3TC monotherapy. b Statistically significant difference between FTC+TDF treated patients and 3TC+TDF treated patients was assessed by Fisher exact test for categorical data and by Wilcoxon test for continuous variables. c Statistically significant differences among the 3 groups of patients were assessed by Chi Squared test for trend for categorical data and by Kruskal Wallis test for continuous variables. PI 2 (0-4) 2 (0-3) 1 (0-2) 0.37 <0.001 Therapy duration (weeks) NE=417 NE=115 NE=55 NE=20 NE=5 NE=6 NE=1 NC=0 NC=140 NC=42 NC=17 NC=9 NC=2 NC=4 • Our study shows a significantly lower prevalence of M184V in FTC+TDF-treated patients than in 3TC+TDF-treated patients and 3TC-treated (TDF-naive) patients. The lower prevalence of M184V is observed in: • - patients receiving a first line HAART • (FTC+TDF: 11.4%, 3TC+TDF: 25.9%, 3TC [naive to TDF]: 51.0%) • as well as • - treatment-experienced patients • (FTC+TDF: 45.9%, 3TC+TDF: 59.4%, 3TC [naive to TDF]: 71.9%). • This result (confirmed by multivariate analysis) may be due to one or more of the following factors: • A greater potency of FTC (Schinazi et al., Antimicrob Agents and Chemother 2005). • A different intracellular pharmacokinetics of FTC-TP versus 3TC-TP (Feng et al., FASEB J1999). • The greater use (in our study) of ritonavir-boosted PI in FTC+TDF-treated patients that, in turn, is associated with a lower rate of mutations in RT at virological failure (Gupta et al., Clinic Infect Dis 2008). • Uni- and multivariate models also suggest that TDF can limit the emergence of M184V (O.R.: 0.60 [95%CI:0.43-0.88], P=0.0085). • Other mutations different than M184V (prevalence, <10% in NRTI-treated patients) may play a role in the in vitro development of resistance to FTC. Clinical confirmation of this observation is warranted. E= event; C= censored The median time to the development of M184V was determined by Kaplan Meier analysis. Statistically significant difference was assessed by Log Rank Test. Low emergence of NRTI resistance mutations in patients failing their first line regimen with FTC+TDF Prevalence of M184V in the subset of 920 3TC (naïve to TDF) treated patients a NRTI-resistance mutations considered are those reported in Johnson et al., HIV Top Med 2008. No mutations associated with transmitted drug resistance mutations were present at baseline. b Statistically significant difference between FTC+TDF treated patients and 3TC+TDF treated patients was assessed by Fisher exact test for categorical data and by Wilcoxon test for continuous variables. c Statistically significant differences among the 3 groups of patients were assessed by Chi Squared for trend for categorical data and by Kruskal Wallis test for continuous variables. d Patients were stratified according to the number of NRTI mutations observed at failure. a The analysis was performed in 920 patients treated with 3TC + other NRTI but not with TDF. b Statistically significant differences were assessed by Fisher exact test. Patients treated with 3TC+ABC are used as reference. c Among them 85 (85.9)patients were treated with AZT, while 14 (14.1) were treated with D4T. Background • Lamivudine (3TC) and emtricitabine (FTC) are structurally related nucleoside reverse transcriptase inhibitors (NRTIs) approved for use in HIV-1-infected individuals. • These two drugs, also in combination with tenofovir (TDF), are frequently proposed as the NRTI backbone of an antiretroviral regimen in both drug-naïve and multi-experienced patients (Hammer et al., 2008). • It is known that both 3TC and FTC select for the M184V/I mutation, resulting in high-level resistance. Nevertheless, few studies have investigated whether: • - the rate of M184V emergence in vivo is different between FTC and 3TC; • - other RT mutations, beyond M184V, are involved in FTC and 3TC resistance. Objective The goal of this study is to investigate genotypic resistance profiles in patients failing therapies containing FTC+TDF, and compare them with 3TC (+ or - TDF). Methods • 1,337 HIV-1 B subtype pol sequences from 168 FTC+TDF-treated patients, 249 3TC+TDF-treated patients, and 920 3TC-treated (naïve to TDF) patients were collected and analyzed. • Factors influencing the emergence of M184V were assessed by multivariate logistic regression (variables considered: subject demographic, length of therapy, drugs co-administered with 3TC/FTC, previous 3TC experience, number of experienced NRTIs). • The association between mutations at baseline and on-treatment was assessed by Fisher exact test. • The phenotypic impact of mutations on FTC resistance was determined using 249 and 111 matched genotype/phenotype pairs collected from the Stanford, and VIRCO databases, respectively.