Download
1 / 68
680 likes | 694 Views
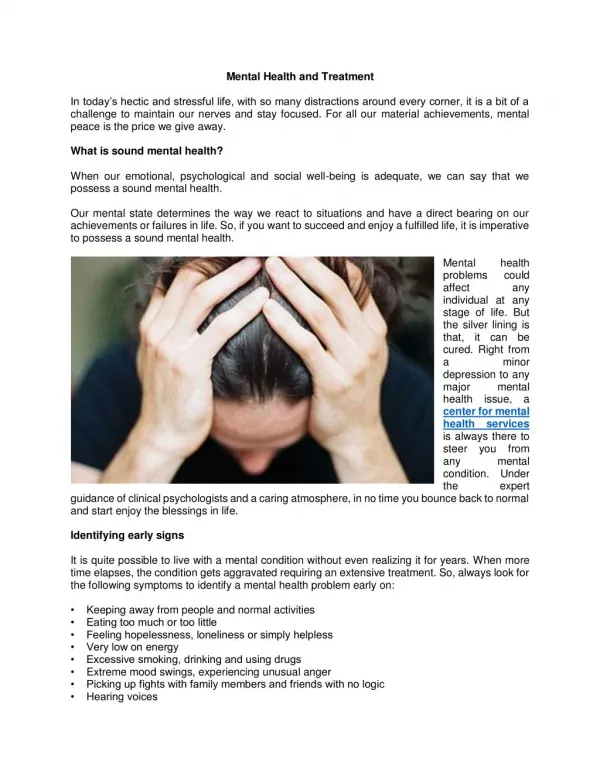
Explore indigenous knowledge & evidence-based practices for integrated mental health care. Addressing youth mental health issues to prevent chronic illnesses effectively.

E N D
The American Indian/Alaska Native National Resource Center for Substance Abuse and Mental Health Services A Strategy for Native Youth Mental Health Treatment and Prevention Services and Programming Dale Walker, MD Patricia Silk Walker, PhD Douglas Bigelow, PhD Bentson McFarland, MD, PhD, Michelle Singer Oregon Health and Science University Tribal Justice and Safety Regional Conference Mystic Lake, Minnesota March 26, 2007
Native Communities Advisory Council / Steering Committee One Sky Center
One Sky Center Partners Tribal Colleges and Universities Cook Inlet Tribal Council Alaska Native Tribal Health Consortium Prairielands ATTC Red Road Northwest Portland Area Indian Health Board One Sky Center Harvard Native Health Program United American Indian Involvement Jack Brown Adolescent Treatment Center National Indian Youth Leadership Project Tri-Ethnic Center for Prevention Research Na'nizhoozhi Center
Goals for Today • An Environmental Scan • Behavioral Health Care System Issues • Fragmentation and Integration • Discuss Mental Health and Comorbidity • Indigenous Knowledge + Evidence Based Knowledge = Best Practice • Integrated care approaches are best for treatment of these chronic illnesses
Five Missions Impossible? • How do we define problems? • How do we ask for help? • How do we get Federal and State agencies to work together and with us? • How do we build our communities? • How do we restore what is lost?
Unipolar Depression Iron-deficiency Anemia Falls Alcohol Use COPD Bipolar disorder Congenital anomalies Osteoarthritis Schizophrenia Obsessive-compulsive disorder 10.7% 4.7 4.6 3.3 3.1 3.0 2.9 2.8 2.6 2.2 Ten Leading Causes of Disability in the World (WHO, 1997)
Males (n = 1,170) Females (n = 656) Type of disorder Prevalence Prevalence Any Listed 66.3 73.8 Conduct Disorder 5.4 3.8 Disruptive Behavior 41.4 45.6 ADHD 16.6 16.4 Affective 18.7 27.6 Anxiety 21.3 30.8 Psychotic 1.0 1.0 Substance Use 50.7 46.8 Juvenile Justice Mental Disorder Rates Chicago Detention Center (Teplin,2002)
Most Common Disabilities Among Youth in the JJ System • Learning Disabilities • Post Traumatic Stress Disorder (higher in girls) * • Conduct Disorder • Oppositional Defiant Disorder • Depression • Anxiety Disorders • Substance Use/Abuse Disorders • Developmental Disabilities
Mental Health Needs: Across Juvenile Justice Placements A study compared mental health needs among a random sample of youth (n=473) within the juvenile justice system found mental health problems in: • 45.9 % of youth on probation, • 67.5% youth incarcerated, and • 88 % youth adjudicated to residential treatment centers (Lyons, Quigley, Erlich & Griffin, 2001)
Native Health Problems Alcoholism 6X Tuberculosis 6X Diabetes 3.5 X Accidents 3X 60% Over 65 live in poverty (US 27%) Depression 3x Violence?
AmericanIndians • Have same disorders as general population • Greater prevalence • Greater severity • Much less access to Tx • Cultural relevance more challenging • Social context disintegrated
Agencies Involved in B.H. Delivery 1. Indian Health Service (IHS) A. Mental Health B. Primary Health C. Alcoholism / Substance Abuse 2. Bureau of Indian Affairs (BIA) A. Education B. Vocational C. Social Services D. Police 3. Tribal Health 4. Urban Indian Health • State and Local Agencies • Federal Agencies: SAMHSA, VAMC, Justice
Disconnect Between Justice/Addictions/Mental Health • Professionals are undertrained • Patients are underdiagnosed • Patients are undertreated • None integrates well with medical and social services
Difficulties of Program Integration • Separate funding streams and coverage gaps • Agency turf issues • Different treatment philosophies • Different training philosophies • Lack of resources • Poor cross training • Consumer and family barriers
Different goals Resource silos One size fits all Activity-driven How are we functioning? (Carl Bell, 7/03)
Best Practice Culturally Specific Outcome Driven Integrating Resources We need Synergy and an Integrated System (Carl Bell, 7/03)
0 Suicide Among ages 15-17, 2001 Death rate per 100,000 2010 Target Females Males Total American Indian White Black Hispanic Asian Source: National Vital Statistics System - Mortality, NCHS, CDC.
Suicide: A Native Crisis Source: National Center for Health Statistics 2001
SUICIDE: A MULTI-FACTORIAL EVENT Psychiatric IllnessCo-morbidity Neurobiology Personality Disorder/Traits Impulsiveness Substance Use/Abuse Hopelessness Severe Medical Illness Suicide Family History Access To Weapons Psychodynamics/ Psychological Vulnerability Life Stressors Suicidal Behavior
Adolescent Problems In Schools 1. School Admin 2. Law 3. FBI 4. DEA 5. State MH 6. State A&D 7. Courts 8. Child Services Alcohol Drug Use Fighting and Gangs Bullying Weapon Carrying School Environment Sale of Alcohol and Drugs Sexual Abuse Unruly Students Truancy Attacks on Teachers Staff Domestic Violence Drop Outs 12
Key Adolescent Risk Factors Aggressive/Impulsive Substance Abuse Depression Trauma
Comorbidity Defined “Individuals who have at least one mental disorder as well as an alcohol or drug use disorder. While these disorders may interact differently in any one person….at least one disorder of each type can be diagnosed independently of the other.” - Report to Congress of the Prevention and Treatment of Co-Occurring Substance Abuser Disorders and Mental Disorders, SAMHSA, 2002
Lifetime History Mental Disorder 22.5% Comorbidity 29% Alcohol Disorder 13.5% Comorbidity 45% Drug Disorder 6.1% Comorbidity 72% Regier, 1990
Lifetime Psychiatric DiagnosesAmong Primary Caretakers (N=207) R. Dale Walker, M.D. (7/97)
Multiple Diagnoses Increase • Treatment seeking • Use of services • Likelihood of no services • Treatment costs • Poor outcome • Suicide risk Dual diagnosis is an expectation, not an exception
The Intervention Spectrum for Behavioral Disorders T r e a t m e n t C a s e I d e n t i f i c a t i o n S t a n d a r d T r e a t m e n t n o f o r K n o w n i Indicated— Diagnosed Youth M t D i s o r d e r s n a e i n v t e r e P n C o m p l i a n c e a Selective— Health Risk Groups n w i t h L o n g - T e r m c e T r e a t m e n t ( G o a l : R e d u c t i o n i n R e l a p s e a n d R e c u r r e n c e ) A f t e r c a r e Universal— General Population ( I n c l u d i n g R e h a b i l i t a t i o n ) Source: Mrazek, P.J. and Haggerty, R.J. (eds.),Reducing Risks for Mental Disorders, Institute of Medicine, Washington, DC: National Academy Press, 1994.
Treatment Brief Intervention Universal/Selective Prevention Spectrum of Intervention Responses Thresholds for Action No Problems Mild Problems Severe Problems Moderate Problems
Ecological Model Society Community/ Tribe Peer/Family Individual
Environmental Interpersonal societal Stigma Community Tribal attitudes Parents Peers National attitudes Personality Attitudes beliefs Genetics Individual Cultural beliefs Schools Local legal Interpersonal State attitudes Personal situations Individual Portrayal in media
Individual Intervention • Identify risk and protective factors counseling skill building improve coping support groups • Increase community awareness • Access to hotlines other help resources
Effective Family Intervention Strategies: Critical Role of Families • Parent training • Family skills training • Family in-home support • Family therapy Different types of family interventions are used to modify different risk and protective factors.
Implications for Treatment • Teach adolescents how to cope with difficulties and adversity • Increase their repertoire of coping strategies • Cognitive therapy is most effective approach
Behavioral Health Programs Should . . . . Reduce Risk Factors • ineffective parenting • chaotic home environment • lack of mutual attachments/nurturing • inappropriate behavior in the classroom • failure in school performance • poor social coping skills • affiliations with deviant peers • perceptions of approval of drug-using behaviors in the school, peer, and community environments
Behavioral Health Programs Should . . . .Enhance Protective Factors • strong family bonds • parental monitoring • parental involvement • success in school performance • prosocial institutions (e.g. such as family, school, religious, and tribal organizations) • conventional norms about drug use
Sources of Strength Access to Mental Health Family Support Positive Friends Access to Medical Spirituality Caring Adults Positive Activities Generosity/Leadership
Effective Interventions for Adults • Cognitive/Behavioral Approaches • Motivational Interventions • Psychopharmacological Interventions • Modified Therapeutic Communities • Assertive Community Treatment • Vocational Services • Dual Recovery/Self-Help Programs • Consumer Involvement • Therapeutic Relationships
Effective Interventions for Youth • Family Therapy • Multisystemic Therapy • Case Management • Therapeutic Communities • Community Reinforcement • Circles of Care • Motivational Enhancement
Treatment Settings - Social Support: A Native Advantage • Tribal • Community • Family • Sibs • Peers • Individual
Cultural Approach • Original Holistic Approach • Psychopharmacology Approach • The unconscious has always been there • Group Therapy • Network Therapy • Recreational / Outdoors • Traditional Interventions • Indian is...
Possible Treatment/Prevention Activities • The Talking Circle • Smudging • Story telling • Traditional Healers • Medicine Person • Herbal remedies • Traditional ceremonies • Sweat Lodge • Traditional Experiences Preservation
Definitions: Indigenous Knowledge • Is local knowledge unique to a given culture or society; it has its own theory, philosophy, scientific and logical validity, which is used as a basis for decision-making for all of life’s needs.
Definitions: Traditional Medicine • The sum total of health knowledge, skills and practices based upon theories, beliefs and experiences indigenous to different cultures…used in the maintenance of health. WHO 2002