Download
1 / 34
360 likes | 604 Views
?. ?. ?. . Olf. system. . LIMBIC SYS. Limbic System: Limbic lobe + hippo., fornix, MMBs, MTT, ant. nuc. thal., cingulate cortex, cingulum, parahippo. gyrus then into hippo. stria terminalis? Papez circuit?. Limbic Lobe. NUTS IN YOUR BRAIN. K-B AND SM .

E N D
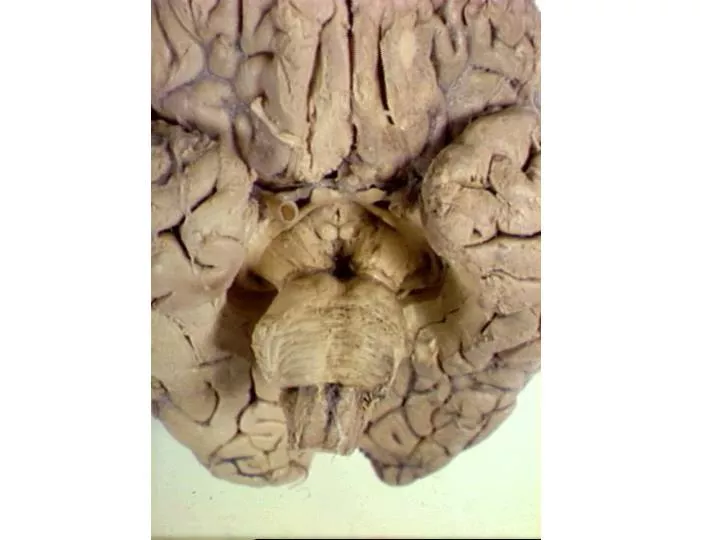
? Olf. system.
LIMBIC SYS
Limbic System: Limbic lobe + hippo., fornix, MMBs, MTT, ant. nuc. thal., cingulate cortex, cingulum, parahippo. gyrus then into hippo. stria terminalis? Papez circuit? Limbic Lobe
NUTS IN YOUR BRAIN K-B AND SM
KLUVER BUCY SYNDROME TAME-no display anger or fear VISUAL AGNOSIA oral compulsions may provide alternate means of object identification HYPERPHAGIC HYPERSEXUAL RECENT MEMORY DEFICIT “Emotional Blunting”
bilateral lesions=Urbach-Wiethe disease=patient SM; insensitivity to the intensity of fear shown by face; hyaline-like deposits skin, muc. memb. does not show autonomic fear responses to arousing stimuli fear learing is lost her memory was not enhanced by emotionally arousing pictures can’t tell negative emotions expressed by other people. Because she often fails to recognize criticism or aggression, S.M. has difficulty interacting socially. no uneasy feeling about someone who is in fact predatorial; does not recognize fear in herself; does not evince normal facial expressions in fearful situations Fear conditioning
programmed by evolution • to detect certain input triggers • important for survival • genetically hardwired • natural triggers • rats are afraid of cats AMYG HPA AXIS BEHAVIOR pain/foot shock bear in woods- smells/sounds-how bear looks ANS Fear conditioning
FEAR CONDITINING! Keeps organism alive!! THAL AMYG HPA AXIS FEAR REACTION sound bear makes river where seen= “learned triggers” Sound bear BEHAVIOR ANS big bear Amyg. org
SENSORY inputs to LATERAL NUCLEUS; then relayed to basal, and accessory basal to reach: • CENTRAL NUC =OUTPUT • CRH receptors on cells and • uses CRH as transmitter to LC adrenal medulla via pregang. sym. • severe CRHventricles
CRH into ventricles=turn on fear response and hypervigilance; • CRH antagonists • central nuc=reduction in the occurrence of above reactions • Target CRHCRH severe Amyg. conn
electrical stimulation? cortisol
CORTISOL CORTISOL CORTISOL CORTISOL
1. cortisol goes up with novelty, uncertainly, threat, conflict, unpredictability, pain, maternal separation 2. cortisol=kills hippo= bad memory and kills PFC= short term memory in depression bad decisions under stress; robs hippo of glucose=toxic effect of glutamate-Cushing’s disease 3. cortisol highest AM and lowest 12 hrs later 4. depression=loss diurnal cortisol levels; elevated Amyghypo
Amygdala projects to hypo: • descending input to T1=L2 • sym.input to adrenal medulla=epi and norepi (hormones) Amyg.LC
PTSD (shell shock!) • NE and CRH = and cortisol = • (cortisol acutely) • increase in cortisol receptors on • ACTH producing cells • exaggerated response to • yohimbine; triggers • flashbacks • decrease in size of hippo • startle response (eye-blink) exaggerated • (Xanax) lowers CRH levels in LC PTSD
PTSD (shell shock!) • horror of a battle is US • sights, sounds smells are conditioned by amygdala • CS can then turn on amygdala • unconsciously and turn on long term memories about original event or recent episodes when trauma was relived • patient listens to tape of traumatic experience MRI activity in amygdala and limbic cortex (especially on right side) low frequency rTMS (repetitive transcranial magnetic stimulation) leads to a decrease in regional cerebral blood flow shocking data
About 16% of American women (about 40 million) are sexually abused (including rape, attempted rape, or other form of molestation) before they reach their 18th birthday. Childhood abuse may be the most common cause of PTSD in American women, 10% of whom suffer from PTSD. learned help..
LEARNED HELPLESSNESS beagles with control over the shock= normal cortisol and NE dog with no control=increased levels of cortisol and DECREASED levels of NE learning that one's behavior is ineffective in changing the environment model for depression dizzi-ing array of connections
Most commonly diagnose anxiety disorder! Panic attacks; sensitive LC-NE system; CO2 turns on solitatrius which turnson LC-NE; Can’t avoid stim like PTSD-internal Yohimbine? LOCUS COERULEUS “blue spot” 19,999 cells?-CCK-agoraphobia? pharmacy
THE PHARMACY • A. monoamine oxidase inhibitors-prevent breakdown of monoamines (catecholamines {epinephrine, norepinephrine, dopamine} and serotonin after release into synaptic cleft • B. tricyclics=prevent REUPTAKE of monoamines back into nerve terminals=imipramine=less side effects • C. SSRIs-selective serotonin reuptake inhibitors=even fewer side effects • D. Roboxetine-selective norepi reuptake inhibitor (SNRI; increases energy) • E. drugs that block ability of CRH to lead to cortisol. • F. circuitry reorganization CA3 and dentate gyrus
THE PHARMACY ANXIETY=25% of all adults; schizophrenia=1%; depression=15% antianxiety drugs work immediately benzodiazepines=Librium, Xanax, Valium= “mother’s little helper” mechanism of action=FACILITATES GABA and makes it harder for glutamate to excite postsynaptic receptors (alcohol and barbituates use this too!)
DEPRESSION Reduction in NE and Serotonin Suicides=5HIAA and MHPG in CSF=Reduced • murderers in Finland low 5-HT • some researchers now believe that suicide may • be the ultimate act of inwardly directed impulsive aggression • depressed had a history of committing impulsive acts including • overeating and aggressive behaviors such as lighting fires or • fighting-5HT low in prefrontal cortex-predict problems
“THE WAY YOU DO THE THINGS YOU DO” Working memory?
HIPPOCAMPUS • cells have receptors for cortisol that may be important in death of such cells-in moderation it increases memory • participates in explicit or declarative memory • lesion results in anterograde amnesia = loss of memories from time of damage on -patient H.M. • patient “RB” showed other closely associated brain areas involved in explicit memory-smaller lesion • loss of synapses and lots of neurofibrillary tangles and senile plaques in Alzheimer’s which leads to problems in explicit memory • cholinergic input to hippocampus is important and one source is nucleus basalis of Meynert = loss of these cells seen in Alzheimer’s (cortical NE low too in Alzheimer’s) • Hippo cells very sensitive to hypoxia
AGING AND THE BRAIN reduction in weight via loss of neurons; few hypothalamic cells lost in comparison with DA cells (sub. nigra., VTA) and NE (LC) lots of cell loss in hippo (20%), cortex, basal forebrain = (nucleus basalis [cholinergic] neurofibrillary tangles in hippo and amyg-cytoskeleton senile plaques in hippo amyg and cortex-extracellular space-betal amyloid protein in young MED I, faces encoded in left PFC and right hippo; recognize faces via right PFC in older (Nsci Profs) no encoding in left PFC and right hippo, but recog. in right PFC. Thus, memory impairment in elderly=no encoding leading to errors in recog.