Download
1 / 26
300 likes | 639 Views
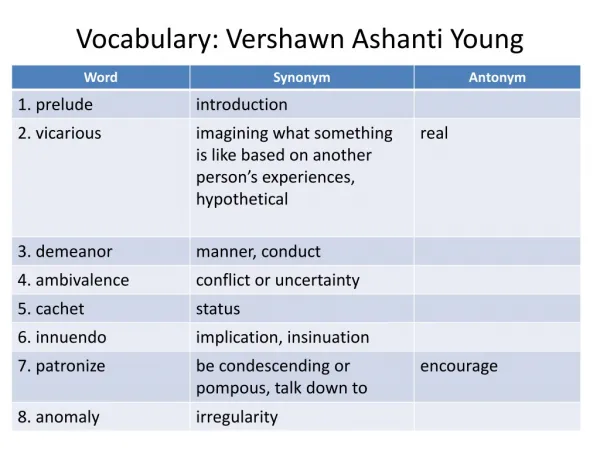
THE SOCIOLOGY OF GENDER AND HEALTH: AN OVERVIEW. Lyn Gardner. DEFINITIONS. Sex – biological or genetic differences between men and women. Largely universal. Gender – socially/culturally constructed differences between men and women. Variable.

E N D
THE SOCIOLOGY OF GENDER AND HEALTH: AN OVERVIEW Lyn Gardner
DEFINITIONS • Sex – biological or genetic differences between men and women. Largely universal. • Gender – socially/culturally constructed differences between men and women. Variable. • Sexism – the personal and institutional differentiation of power and status between the sexes which limit opportunities for girls and women. • Gender/sex role – pattern of behaviour a particular society expects from individuals of either sex. Learned through socialisation.
Recognising the Social Construction of Gender ‘Gender refers to women’s and men’s roles and responsibilities that are socially determined. Gender is related to how we are perceived and expected to think and act as women and men because of the way society is organised, not because of our biological differences’. Gender and Health, WHO (1998:5)
THE SECOND SEX ‘In truth, to go for a walk with one’s eye open is enough to demonstrate that humanity is divided into two classes of individuals whose clothes, faces, bodies, smiles, gaits, interests and occupations are manifestly different. Perhaps these differences are superficial, perhaps they are destined to disappear. What is most certain is that they do most obviously exist.’ Simone De Beauvoir – 1953
SOCIAL EXPLANATIONS OF GENDER DIFFERENCES • Feminine traits are de-valued and under-valued by society. • Women as relative beings – ‘woman as other’. In a very important sense, it is normal to be a man and abnormal to be a woman
Explanations Cont. • The process of socialisation places men in a different position to women: a masculine archetype • Traditional notions of masculinity position men as ‘breadwinners’, risk takers (in terms of hazardous work – industrial accidents, contact with harmful substances, and other pursuits such as sport, sex, violence and health damaging behaviours – smoking and excessive alcohol intake) See Doyal, L. (2002) in Bendelow, G. et al (eds) Gender, Health and Healing. London:Routledge.
GENDER SOCIALISATION TAKES PLACE IN: the family school/education media wider society
FAMILY • Do parental/family expectations of boys and girls push them into particular gender roles? • Gender stereotypes: girl babies are quiet, clean and restrained. Boys are noisy and adventurous. • Research into reactions to a crying baby: told it was a boy – interpret as anger. Told it was a girl – interpret as fear. • Promotion of emotional inhibition (‘big boys don’t cry’), positive sanctions (‘what a brave boy’) and prohibition of feminine behaviour (‘don’t be a woos’) See Stillion (1995) • Or are parents/families responding to initial differences in behaviour?
SCHOOL • Teacher expectations may be different. • ‘Hidden curriculum’ – guides pupils’ expectations and behaviour. • Evidence to suggest that boys get more attention from teachers. • Peer pressure to conform to particular gender roles or stereotypes. • Recent challenges to traditional male role = uncertainty for boys/young men • Role models (or lack of) may influence subject/course choice
MASS MEDIA INFLUENCES • Portrayal of women as either ‘sexual objects’ or caring/nurturing. • Emphasis on women’s appearance. • ‘You’re only a feminist because you’re ugly!’…. • Treatment of women who commit violent crimes – ‘doubly deviant’ – a crime against your sex (gender?).
Health Surveillance: a Foucauldian Perspective • The medical gaze – societal gaze • The process of observation, or surveillance, by both the medical profession and wider society – whereby individuals are measured against a given masculine or feminine benchmark • Individuals assess their performance in a process of self-surveillance • Yet men have an uneasy relationship with their bodies and health (see White, A.K. and Johnson, M. (2000) Men making sense of chest pain in J. of Clinical Nursing, 9:534-541. • ‘The maintenance of the male body becomes problematic’ (White and Johnson, p.535)
Social or Biological? ‘Men’s health is not a medical issue, it is societal’ argues White (2001:3) Yet equally, argues Doyal (2002), this is the case for women also – both nationally and globally.
DIFFERENCE/SAMENESS DEBATE • Why should any difference – if it exists, or we believe it to – be constructed as disadvantage, particularly for women? • If we are the same – the problem of women's relative disadvantage and lack of power remains unresolved. • What needs to be addressed is not are we the same or different, but what structures exist which convert this into disadvantage?
LEGISLATION TO ADDRESS SEXUAL INEQUALITY • 1882 Married Women’s Property Act • 1919 Votes for Women over 30 • 1923 Equality in grounds for divorce • 1928 Votes for women over 21 • 1970 Equal Pay Act • 1975 Sex Discrimination Act • 1992 Church of England Synod votes to allow women priests
Contemporary Social Changes in the Lives of Men and Women • Changes in work and employment: ‘Women are almost as likely as men to be employed; but almost all of this increase is in part-time work. There has been a significant narrowing of the wages gap between women and men who work full-time, but this does not extend to women who work part-time. There has been a major increase in the proportion of women in top jobs, but significant sex segregation in employment still remains’. Walby, 1997:36-7).
Cont. • Changes in educational achievement: there is evidence that women have made (and continue to make) rapid gains in educational terms since the mid-1980s, in comparison to their male counterparts. A larger increase in admissions to HE (115% over a 10 year period, compared to only 35% increase for men), improvements for girls in GCSE and A level achievements.
Cont. • Changes in family and household: fertility rates (falling birth rate), rise in single-parent households (estimates suggest 90% of these are women-headed), increase in divorce rate. • Yet women still maintain the majority share of household tasks and childcare (and other care) responsibilities • Increase in older, single/widowed households (risk of poverty – feminisation of poverty)
GENDER & HEALTH INEQUALITIES ‘Women get sicker but men die quicker’ (Miers, 2000) Morbidity rates are higher for women Mortality rates are higher for men
Statistically Speaking… • Life expectancy is higher for women than men: in 2001 life expectancy at birth for women was 80.4 years compared with 75.7 for men. • Life expectancy for men has been increasing faster than for women: an increase of 4.8 years for men, and 3.6 years for women between 1981 and 2001.
More stats… • In 2001 obesity levels were similar for both sexes: nearly half of men were considered overweight, compared with a third of women • Underweight: men 4%, women 6% • Men twice as likely to exceed recommended daily benchmarks for alcohol consumption (3-4 units daily for men, 2-3 for women) • Young men more likely to binge drink • Student drinking levels/behaviours revealed no significant differences between the sexes!
CRITIQUE • THE PICTURE IS MORE COMPLEX • Gender differences are less significant in middle years of life – age ranges are significant. • Men have higher rates of serious illness than women • Women have higher consultancy rates than men – particularly GP contact • When consultations for pregnancy/childbirth and GU are removed, gender differences are less significant
The New Woman – Emancipation Thesis • Women are increasingly consuming alcohol in larger quantities – and drinking more frequently • Women are smoking in greater numbers than before • Women are more at risk from injuries at work (in addition to higher risk of injury in the home) • Increasingly more likely to indulge in ‘risk-taking behaviours’ which may be damaging to health • Increasingly more likely to be injured or killed in road and car accidents
WHY ARE WOMEN THE MAIN CONSUMERS OF HEALTH CARE? • WOMEN ASSUME MAIN RESPONSIBILITY FOR CONTRACEPTION • WOMEN ENCOUNTER MEDICAL PROFESSION DURING PREGNANCY AND CHILDBIRTH • WOMEN ASSUME PRIME RESPONSIBILITY FOR WELL AND SICK CHILDREN • WOMEN’S ANATOMY IS SEEN TO BE MORE COMPLEX THAN MEN’S AND APPEARS TO BE MORE LIKELY TO SUCCUMB TO HELATH PROBLEMS AND ILLNESS • TRADITIONALLY WOMEN HAVE BEEN SEEN TO BE FRAIL – MEDICINE HAS CAPITALISED ON WOMEN’S PERCIEVED WEAKNESSES ( FROM THE VAPOURS TO PMS) • WOMEN SEE THEMSELVES AS ILL MORE OFTEN THAN MEN
WOMEN AND MENTAL ILLNESS Historically women have been admitted to psychiatric hospital at a higher rate than men – in 1999 468 per 100,000 – men 364 per 100,000 Women are twice as likely to be taking tranquillisers Two-thirds of people taking anti-depressants are women Women are the majority recipients of ECT (approx 70%) But the picture is changing as the psychiatric services focus resources on the people experiencing the so-called serious and enduring mental illnesses e.g. Schizophrenia, Bi-polar Disorder Why should this impact on care provision for women?
Impact on Health Women may still (just) have some advantage over men in life expectancy, may seem to get ‘sicker’ (higher rates of morbidity), may be protected to some extent from CHD due to oestrogen levels – but their changing patterns of behaviour are giving cause for interest and concern: women are becoming more like men, and thus experiencing similar health problems.
Suggested Reading • Annandale, E. & Hunt, K. (2000) Gender Inequalities in Health. OUP: Buckingham. • Busfield, J. (1996) Men, Women and Madness. Macmillan: Basingstoke. • Doyal, L. (1995) What Makes Women Sick? Macmillan: Basingstoke. • Miers, M. (2000) Gender Issues and Nursing Practice. Macmillan: Basingstoke. • Wilkinson, S. & Kitzinger, C. (eds) (1994) Women and Health: Feminist Perspectives. London: Taylor and Francis. • National statistics online • Davidson, N. and Lloyd, T. (eds) (2001) Promoting Men’s Health. London: Bailliere Tindall. • www.menshealthforum.org.uk • Social Science and Medicine (1999, 4, 1) special issue on gender and health.