Download
1 / 21
220 likes | 301 Views
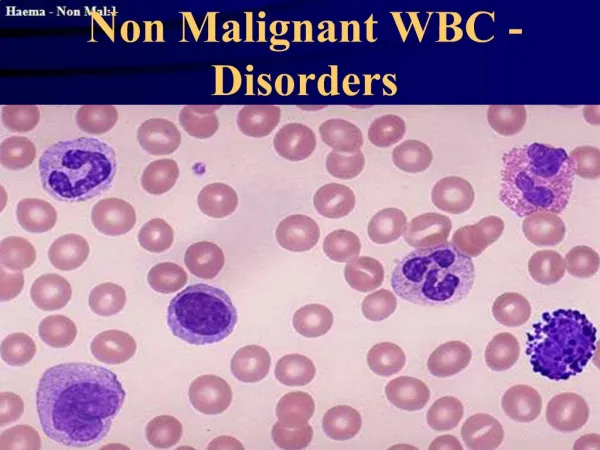
Non leukemic myeloproliferative disorders. polycythemia vera(PV) Non leukemic Essential thrombocythemia (ET) Myelofibrosis(MF). myeloproliferative disorders(MPD).

E N D
Nonleukemicmyeloproliferative disorders polycythemia vera(PV) Non leukemic Essential thrombocythemia (ET) Myelofibrosis(MF)
myeloproliferative disorders(MPD) a group of conditions characterized by clonal proliferation of one or more haemopoietic components in the BM & in many cases in the liver & spleen. These disorders are closely related to each other , transitional forms occur & in many cases an evolution from one entity into other occurs during the course of disease.
polycythemia vera(PV), polycythemia rubra vera(PRV) blood changes includes an increased haemoglobin above 17.5 g/dl in adult males & 15.5 g/dl in females usually with increased red cell count above 6×109 /l in male & 5.5×109 /l in females & haematocrit above 55% in males & 47% in females . The increased in red cell volume is caused by endogenous myeloproliferation due to stem cell defect, so in many patients overproduction of granulocytes & platelets occur as well as of red cells.
Clinical features: This disease is of old subjects with equal sex incidence & the clinical features are the result of hyperviscosity, hypervolaemia or hypermetabolism. 1-Headach, pruritis (especially after hot path) , dyspnoea, blurred vision & night sweat. 2- Plethoric appearance – ruddy cyanosis . 3- Splenomegaly in 2/3 of patients. 4-Haemorrhage or thrombosis ( either arterial or venous ). 5- Hypertension in 1/3 of patients. 6- Gout due to raised uric acid production 7- Peptic ulceration in 5-10%.
Lab. Findings: 1-The haemoglobin, haematocrit, red cell count & total red cell volume are increased. 2-Neutrophil leucocytosis is seen in 1/2 0f cases. 3-Raised platelets count in 1/2 of cases. 4- The neutrophil alkaline phosphatase score is high. 5- Increased serum B12 & B12 binding capacity because of increased transcobalamin 1 6- BM: is hypercellular with prominent megakaryocytes . 7-Blood viscosity is increased. 8- Plasma urate is often increased. 9- Circulating erythroid progenitors are increased & grow in vitro independently of erythropoietin.
Essential thrombocythaemia (ET), primary thrombocythaemia Megakaryocyte proliferation & overproduction of platelets count above normal ,this condition is closely related to PRV .Some cases show patchy fibrosis.
Criteria for diagnosis of ET: Platelets >600×109 /L No evidence or indication of raised red cell mass No Philadelphia chromosome or bcr-abl rearrangement No support for a diagnosis of MF No demonstrated cause for reactive thrombocytosis
Clinical features: 1-Recurrent hemorrhage & thrombosis 2- splenic enlargement in early phase but splenic atrophy due to platelets blocking the splenic microcirculation 3- There may be anemia (due to iron deficiency anemia from chronic bleeding) or polycythaemia Lab. Findings: 1-Abnormal large platelets & megakaryocyte fragments may be seen in peripheral blood film 2-The BM is similar to that in PRV 3-Cytogenetic are analyzed to exclude CML 4-Platelet function tests are constantly abnormal ( Failure of aggregation with adrenaline)
Myelofibrosis(MF) Pathogenesis: Generalized haemopoietic stem cells proliferation with splenic & hepatic involvement in which there is extramedullary haemopoiesis , there is reactive fibrosis in BM secondary to hyperplasia of abnormal megakaryocytes. There is stimulation of fibroblast probably by platelet-derived growth factor secreted by megakaryocytes & platelets & inhibition of collagenase by platelet factor IV.
Clinical features 1- 1/3 of patients has previous history of PRV & some times present with features of both disorders. 2- An insidious onset in older people is usual with symptoms of anemia 3-Symptoms due to massive splenomegaly 4- loss of weight, anorexia & night sweats are common. Bleeding problems, bone pain, gout occur in minority of patients.
Lab. Findings: 1-Anemia is usual but normal or increased hemoglobin may be found in some patients. 2- The WBCs & platelets count are frequently high at the time of presentation, later in disease leucopenia & thrombocytopenia are common 3- A leuco-erythroblastic blood film is found .The red cells show characteristic tear drop shape. 4- BM is usually not obtainable by aspiration .Trephine biopsy may show hyper cellular marrow with increased reticulin-fiber pattern.
Other causes of marrow fibrosis: 1-CML 6- Metastatic carcinoma 2- AML FAB7 7- Non-Hodgkin's lymphoma 3-MDS 8--Hodgkin's disease 4- myeloma 9- Tuberculosis 5- Hairy cell leukemia 10- Leishmaniasis
Multiple myeloma(MM) Is neoplastic monoclonal proliferation of BM plasma cells. Characterized by lytic bone lesion, plasma cell ,accumulation in BM & presence of monoclonal protein in serum & urine. 98% of cases over the age of 40, with peak incidence in the 7th decade
Clinical features 1- Bone pain, pathological fracture. 2- Features of anemia. 3- Repeated infections because of deficient Ab & later on because neutropenia. 4-features of renal failure & /or hypercalcaemia . 5- Abnormal bleeding tendency because myeloma protein interfere with platelets function & coagulation factors & later on because of thrombocytopenia. 6- Occasionally macroglossia , carpal tunnel syndrome, diarrhea due to amyloid disease 7- In 2% hyperviscosity syndrome.
Diagnosis ( Lab. Findings) : This depends on 3 principle findings 1- In 98% of patients monoclonal protein occurs in the serum or urine or both. The serum paraprotein is IgG in 2/3 of cases. The urine contain Bence-Jones protein in 2/3 of cases which is free light chains ( κ or λ) of the same type of serum paraprotein 2- BM shows increased plasma cells > 4% & usually > 30% often with abnormal form ( myeloma cells) , these cells are monoclonal B cells & express the same Ig heavy & light chain of serum monoclonal protein
3- Skeletal survey shows osteolytic areas without evidence of surrounding ostublastic reaction. Usually at least 2 of the 3 diagnostic features mentioned above are present.
Other lab. Findings: 1-Normochromic ,normocytic anemia . Rouleaux formation is marked in most cases .Neutropenia & Thrombocytopenia in advanced cases .Plasma cell seen in blood film in 15 % of cases. Leucoerythroblastic picture occasionally seen. 2- High ESR( Erythrocyte sedimentation rate.) 3- Serum calcium increased in 45% of patients. 4-Blood urea & serum creatinine increased in 20% if cases. 5- Low serum albumin occurs in advanced disease.
Plasma cell leukaemia: This occurs either as a late complication of myeloma disease or often in younger patients as a primary disease characterized by the presence of 20% or more plasma cells in the blood, with an absolute count of>2×109/L . There is more liver & spleen involvement than in myeloma, the paraprotein concentration in serum is often low .The results therapy is poor.