Download
1 / 12
140 likes | 913 Views
Bleb leak characteristics and success of repair following trabeculectomy with Mitomycin C. Amy Hennessy, MD MPH Harold Bernstein, MD Medical College of Virginia Richmond, VA Authors have no financial interests to disclose. Background.

E N D
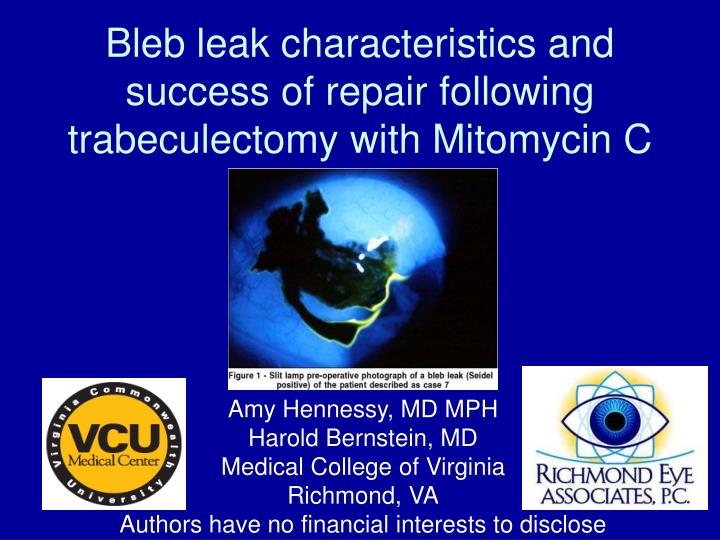
Bleb leak characteristics and success of repair following trabeculectomy with Mitomycin C Amy Hennessy, MD MPH Harold Bernstein, MD Medical College of Virginia Richmond, VA Authors have no financial interests to disclose
Background • Mitomycin C and 5-fluorouracil are the most common adjunctive agents used in filtering surgery today • Blebs may be thinner with more irregular epithelium, breaks in basement membrane, fewer goblet cells, and atrophic and avascular stroma 1,2,3,4,5 • Thin, avascular, leaking blebs commonly associated with blebitis or endophthalmitis 1,2,3,4
Bleb leaks are relatively common and can be potentially serious • 4.2-10% incidence of late bleb leak after trabeculectomy with MMC5 • Risk of bleb leak, blebitis or endophthalmitis during the first 5 years after trabeculectomy is 4.4% per year1 • 3 times greater incidence of bleb leak in eyes treated with MMC compared with eyes treated with 5-FU (5.9% vs 1.7%)5 • In a group of 123 eyes of POAG patients followed for 6.8 years after trabeculectomy, 9 with bleb leak, 4 with blebitis6 • In 258 trabeculectomies DeBry and colleagues identified 9% incidence of bleb leak; 2% blebitis, 3% endophthalmitis1 • Infection 25 times greater in eyes with bleb leaks compared to those without leak7
Bleb leak management Goal: • Eliminate leak and hypotony while preserving filtration function and maintaining target IOP 2,7,8 Surgical bleb leak management: • Conjunctival advancement with or without excision of the existing bleb, free conjunctival graft, scleral patch graft, amniotic membrane graft2,3,4,7,9 • 2 most frequent techniques: free conjunctival graft and advancement of adjacent conjunctiva4,7,9 • Best surgical approach unclear2
Purpose of Study • Characterize a population of patients who experience bleb leaks following trabeculectomy with mitomycin C • Determine predictors of successful outcome of surgical repair by 1 surgeon • Determine outcomes (visual acuity, IOP, Seidel status) before and after typical conjunctival advancement repair of bleb leak
Methods • Retrospective medical record review of 16 patients with documented bleb leaks found over a 3 year period • At least 1 month of post-operative follow-up • 2 with associated blebitis • SAS statistical program used to analyze data • Initial conservative treatment (aqueous suppression, bandage contact lens, topical antibiotic, eye shield) followed by surgical repair: 2 possibilities • If mobile conjunctiva and bleb not extending onto cornea, then conjunctival advancement with cautery to de-epithelialize thin conjunctiva (10/16) – If need for bleb excision or patch graft required, more difficult repair performed, sometimes including entry into anterior chamber (6/16)
Definition of successful repair • No blebitis, no endophthalmitis, no bleb dysesthesia • Resolution of leak • No further surgery • < 1 additional IOP-lowering med • IOP maintained between 6 and 21 • Grading success: • “Complete” success: • All criteria met; no surgery or medical problems post-op • “Partial” success: • No return to surgery, no infection, no dysesthesia but additional meds required to maintain IOP between 6 and 21 • Failure: • Return to surgery • Need for 2 or more medications for IOP control
Results • 16 patients with bleb leak • 9 male (56.25%), 9 white (56.25%) • Average age at initial surgery 66.6 (+9) years • 15 POAG, 1 unintentional filtering bleb (ICCE) • 14 trab, 1 combined procedure • All 15 received MMC with initial trabeculectomy • Mean concentration 0.5mg/cc • Mean duration 1.8 minutes • 68.75% limbal-based flap, 3 unknown, 1 fornix-based • Average age at leak 74.3 (+7.9) years • Mean of 95.4 months (~8 years) from initial surgery to leak • Surgical repair 6.1 months after leak noted • Range 21 days-21 months • Given 2-3 office visits with non-surgical measures • Large range of delayed repair due to patient issues • Refused surgery, not medically stable
Results • Mean follow-up after repair: 8.1 months +/- 4.7 (range 1 month to >12 months) • Intraocular pressure significantly increased (p<0.0001) • Pre-op IOP 5.3 + 4.1 (range 0-15) • Post-op IOP 12.6 + 3.4 (range 6-21) • Visual acuity improved (p=0.09) • Mean pre-op logMAR 0.56 (VA 20/70) • Mean final post-op logMAR 0.33 (VA 20/40)
Success of repair • Complete success: • 11/16 (68.75%) • At least “Partial” success: • 14/16 (87.5%) • Failure: 2/16 (12.5%) • IOP 27 on 4 medications • Persistent leak • No clinical factors predicted success or failure • 5-FU not given in post-op period may be associated with failure (OR 4.8, CI 0.4-58.0) (p=0.21)
Conclusions • Bleb leak is an infrequent yet significant problem complicating filtering surgery • This small study on bleb leak repair shows similar results to studies by Catoira 2 and Tannenbaum 8 • Bleb repair by conjunctival advancement appears successful in correcting bleb leak, maintaining IOP, improving visual acuity and preventing bleb-related infection when other methods have failed • It may be that 5-FU given in post-operative period affects the outcome of bleb leak repair
References • 1. DeBry PW, Perkins TW, Heatley G, Kaufman P, Brumback LC. Incidence of late-onset bleb-related complications following trabeculectomy with mitomycin. Arch Ophthalmol. 2002 Mar; 120: 297-300. • 2. Catoira Y, WuDunn D, Cantor, LB. Revision of Dysfunctional filtering blebs by conjunctival advancement with bleb preservation. Am J Ophthalmol. 2000; 130: 574-579. • 3. Wadhwani RA, Bellows AR, Hutchinson BT. Surgical repair of leaking filtering blebs. Ophthalmology. 2000 Sep; 107(9): 1681-1687. • 4. Budenz DL. Barton K, Tseng SCG. Amniotic membrane transplantation for repair of leaking glaucoma filtering blebs. Am J Ophthalmol 2000; 130: 580-588. • 5. Greenfield DS Liebman JM Jee J Ritch R. Late Onset bleb leaks after glaucoma filtering surgery. Arch Ophthalmol. 1998 April; 116: 443-447. • 6. Shigeeda T, Tomidokoro A, Chen YN, Shirato S, Araie M. Long-term follow-up of initial trabeculectomy with mitomycin C for primary open angle glaucoma in Japanese patients. J Glaucoma. 2006 Jun; 15(3): 195-199. • 7. Burnstein AL, WuDunn D, Knotts SL, Catoira Y, Cantor LB. Conjunctival advancement versus nonincisional treatment for late-onset filtering bleb leaks. Ophthalmology. 2002 Jan; 109(1):71-75. • 8. Tannenbaum DP, Hoffman D, Greaney MJ, Caprioli J. Outcomes of bleb excision and conjunctival advancement for leaking or hypotonous eyes after glaucoma filtering surgery. Br J Ophthalmol. 2004 Jan; 88(1): 99-103. • 9. Budenz DL, Chen PP, Weaver YK. Conjunctival advancement for late-onset filtering bleb leaks: indications and outcomes. Arch Ophthalmol. 1999 Aug; 117(8):1014-1019.