Download
1 / 25
250 likes | 394 Views
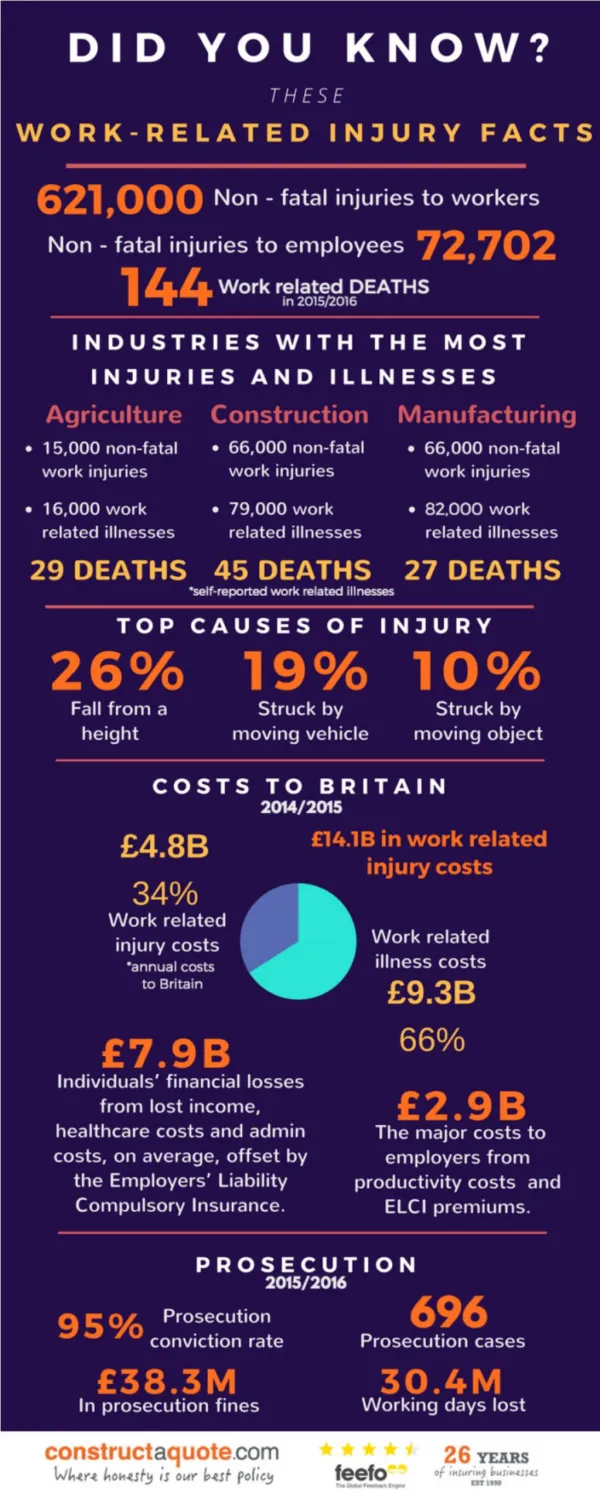
Opioid Use in Work-related Injuries. Pacific Northwest Chapter - Association of Occupational Health Professionals (AOHP) January 4, 2011. Jaymie Mai, PharmD Pharmacy Manager. A Historical Perspective.

E N D
Opioid Use in Work-related Injuries Pacific Northwest Chapter - Association of Occupational Health Professionals (AOHP) January 4, 2011 Jaymie Mai, PharmD Pharmacy Manager
A Historical Perspective • Prior to 1996, prohibition on opioid use for chronic non-cancer pain led to under-treatment • New permissive regulations allow more aggressive treatment of pain with opioids • WA DOH Guidelines for Management of Pain1998 • L&I Guidelines for Outpatient Prescription of Oral Opioids for Injured Workers with Chronic, Non-cancer Pain 2000
L&I 2000 Guideline - Oral Opioids for Injured Workers • Payment as long as there is substantial reduction in pain & ongoing improvement in function (WAC 296-20-03022) • Emphasizes use of best practices and focuses on rehabilitation (WACs 296-20-03019 through 03024)
Documentation Requirements for Opioids • Initiating opioids for chronic, non-cancer pain • Initial report (billing code 1064M) • Opioid progress report (billing code 1057M) • Treatment agreement • Ongoing opioid treatment • Opioid progress report every 60 days • Treatment agreement every 6 months • Functional progress form (optional)
Emerging data on mortality, morbidity & dose-related risk with chronic opioid use
Age-adjusted rate per 100,000 population 3.1-9.0 9.1-11.4 11.5-21.1 Unintentional & Undetermined Opioid Overdose Death Rates by State 2007 Source: Centers for Disease Control and Prevention
Washington Opioid Deaths & Sales of Rx Opioids Source: Washington State Department of Health
Washington Hospitalizations from Opioid Overdose 1987 - 2008 Source: Washington State Department of Health
L&I Dosing Trend of Long-acting Opioids (morphine equivalent dose)
1st to validate association between specific dose levels and severe overdose events Risk of morbidity and mortality increased 8.9 fold at 100mg/d of morphine equivalent dose (MED) 7 non-fatal overdose events for each death Editorial by Dr. McLellan (White House Office of National Drug Control Policy): “Smarter, more responsible (prescribing) practices are the only hope to avoid tragic, avoidable deaths” Group Health Study Source: Dunn et al. Ann Int Med 2010;152:85-92
Severe Opioid Complications • Sleep apnea • 92% prevalence of ataxic or irregular breathing during NREM sleep at >/= 200 mg MED (Walker et al. J Clin Sleep Med 2007;3:455-61) • Endocrine dysfunction – testosterone deficiency • Addiction • Rate up to 18.9% (Fishbain et al. Clin J Pain 1992;8:77-85) • Hyperalgesia • Abnormal pain sensitivity with chronic opioid use (Ballantyne J. Pain Physician 2007;10:479-91) • Disability
Early Opioid Use and Low Back Disability • During the first 6 weeks of low back injury: • Opioids >7 days significantly associated with disability in 1 year • ≥2 opioid prescriptions doubled the odds of 1-year disability • >150mg total morphine equivalent dose (MED) prescribed was associated with doubling of 1-year disability Source: Franklin et al. Spine 2008;33(2):199-204
Best Practices When Prescribing Opioids • Do initial evaluation & assessment • Physical examination, comprehensive assessment • Screen for risk • Addiction, abuse or aberrant behavior; psychiatric status • Check state’s prescription monitoring program (PMP) if available or other systems such as the emergency department information exchange (EDIE) • Establish treatment goals or plans • Define effectiveness (improve function & pain); monitor risks, adverse effects, complications; single prescriber & pharmacy • Sign treatment agreement or informed consent • Discuss risks, benefits, complications; patient expectations; random urine drug testing
Best Practices When Prescribing Opioids • Monitor treatment • Ongoing assessment of effectiveness by tracking pain and function and adverse effects or complications; random urine drug testing; psychiatric co-morbidities • Periodically check the state’s PMP if available and other systems such as EDIE • Dosing guidance • Know how to calculate total morphine equivalent dose • Reassess at 100 - 120mg/d MED if pain and function have not improved; consider alternative treatment or consultation • Taper or discontinue treatment • When function or pain does not improve after trial; significant adverse effects; misuse, addiction or diversion
Opioid dose calculator Screening tool for alcohol and substance abuse 2-question tool for tracking pain and function Patient education aids Detailed advice on using urine drug testing to screen risk and monitor compliance Additional Tools Available Through AMDG For more on the AMDG Opioid Dosing Guideline, go to http://www.agencymeddirectors.wa.gov/default.asp
New efforts to reduce opioid-related mortality and morbidity
Health Care Providers Use opioids only after alternatives failed and lowest effective dose In addition to behavioral screening and use of patient contracts, consider random, periodic, targeted urine testing If a patient’s dosage has increased to ≥120 morphine milligram equivalents per day without substantial improvement in pain and function, seek a consult from a pain specialist Do not prescribe long-acting or controlled-release opioids for acute pain Periodically request a report from your state prescription drug monitoring program For complete recommendations, go to http://www.cdc.gov/HomeandRecreationalSafety/pdf/poision-issue-brief.pdf New CDC Recommendations
FDA Risk Evaluation and Mitigation Strategies (REMS) for Opioids • Ensure benefits of drug outweigh risks • All extended release oral opioids (hydromorphone, morphine, oxycodone, oxymorphone); methadone for pain; transdermalfentanyl • Proposed REMS include (July 2010) • Medication guides • Elements to Assure Safe Use (EASU) for prescribers education • Mandatory sponsor-developed patient educational materials available to providers for voluntary use with patients • Advisory committee did not agree with the FDA proposed REMS
AMDG Opioid Dosing Guideline • Collaboration with clinical and academic pain experts • Improve care and safety with opioid treatment through use of “best practices” • Consult before exceeding 120mg/d MED if pain and function have not improved • Assist provider in optimizing opioid treatment for patients who are above the dosing threshold For more on the AMDG Opioid Dosing Guideline, go to http://www.agencymeddirectors.wa.gov/default.asp
Repeals existing WACs New WACs by June 2011 with guidance on Dosing criteria Consultations and ways for electronic consultation Tracking clinical progress with tools (pain interference, physical function, overall risk for poor outcome) Tracking use of opioids Exempt acute pain, palliative, hospice or other end-of-life care ESHB 2876 – Pain ManagementChapter 209, Laws of 2010