Download
1 / 63

E N D
Pt.1 K.Gu.- Clinical presentation • K.G. was a 59 y.o. female in 1990 when she noted the development of enlarged lymph nodes in her left inguinal region. A lymph node biopsy yielded a diagnosis of lymphoma, and subsequent staging yielded evidence of periaortic, bilateral inguinal, and bilateral axillary lymph node involvement, and bone marrow infiltration. • In 1994, the patient noted enlargement of a right inguinal lymph node, and another lymph node biopsy was performed.
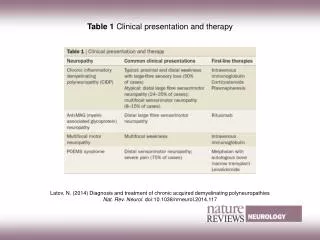
Indolent Small lymphocytic lymphoma/CLL Follicular lymphoma, Grades 1/2 Extranodal Marginal zone lymphoma of MALT type Nodal marginal zone lymphoma Splenic marginal zone lymphoma Hairy cell leukemia Lymphoplasmacytic lymphoma Plasma cell myeloma Plasmacytoma Cutaneous T cell lymphoma Cutaneous CD30+ anaplastic large cell lymphoma Aggressive Prolymphocytic leukemia Large B cell lymphoma Burkitt lymphoma Mantle cell lymphoma Anaplastic large cell lymphoma All peripheral T cell lymphomas Indolent versus aggressive Divides B and T
Pt K.G. Diagnosis: 1990: Follicular lymphoma, Grade I • Therapy 1990 • Prognosis 1990
Pt. K.G. Diagnosis: 1990:Follicular lymphoma, Grade I1994: Progression to diffuse large cell lymphoma • Therapy 1994 • Prognosis1994 • Clinical follow-up
K G. lessons • Follicular lymphomas are the second most common type of lymphoma seen in Western countries • Most are disseminated at diagnosis, Stage III or IV • In the most common forms, Grades 1 and 2, they are indolent lymphomas • Mean survival >7 years • Pathogenesis due to failure of apoptosis, programmed cell death • Caused by translocation, t(14;18)(q32;q21) • Produces constitutive expression of Bcl2, an anti-apoptotic protein, so cell immortalized, but small replicating fraction and slow growth of tumor • Therapy during indolent phase based on age, stage, symptoms • Until recently, felt to be incurable, but controllable • Watch and wait vs limited chemotherapy vs transplant • Can progress to large cell lymphoma • More aggressive disease due to activation of cell cycle mechanism • Now increased growth fraction plus defective cell death • Requires more aggressive multiagent chemotherapy vs transplant
K. G. Lessons 2 • Large B cell lymphoma can present de novo • Most common type of lymphoma in Western countries • Classic type of aggressive lymphoma, a disease of excessive cell growth and replication • Morphologic manifestation is large cell with “vesicular” chromatin pattern and prominent nucleoli, and increased mitoses • Median survival in absence of effective therapy less than 2 years • Most will respond to aggressive, multiagent therapy • Overall, 60% will relapse, 40% can be cured
K G-lessons • Prognostic factors in diffuse large cell lymphoma: • International Prognostic Index factors • Age • Stage • LDH level • Number of extranodal sites • Performance score
K G.-lessons • Prognostic factors in diffuse large cell lymphoma: • International Prognostic Index factors • Age • Stage • LDH level • Number of extranodal sites • Performance score • Biologic predictors • Cytogenetics • Upregulated proteins • Microarray pattern • Follicular center cell phenotype • Activated B cell phenotype
Pt.2 S.N.- Clinical presentation • S.N. was a 56 y.o. male in May, 1996 when he noted the onset of fever, night sweats, and weight loss. Physical examination revealed splenomegaly and a right upper quadrant mass. Radiologic study and MRI revealed mediastinal lymph nodes and jejunal thickening. A CBC revealed a WBC of 12,000, with 50% atypical lymphocytes. A laparotomy was performed at an outside hospital, with lymph node and liver biopsies. A bone marrow study was subsequently performed at DHMC.
Pt. SN- Diagnosis: mantle cell lymphoma • Therapy 1996 • Current therapy approach • Prognosis 1996 • Clinical follow-up • Lessons-the indolent lymphoma imitator
>70% 5 yr. surv 50-70% 5 yr. surv 30-49% 5 yr. surv <30% 5 yr. surv
Patient JC JC is a 22 yo male who presented to his local MD in March, 2001 with severe back spasms, initially treated with NSAIDS. He then developed increasing abdominal and left shoulder pain, fatigue, and 15 lb weight loss over the next six weeks, followed by night sweats seven days before admission to DHMC. Initial chest and abdominal X-rays at an outside hospital were negative, but a subsequent abdominal CT scan detected a retroperitoneal mass estimated at 18x11x8.5cms and a smaller soft tissue mass in the right anterior abdomen. Chest CT revealed bilateral axillary adenopathy. The abdominal wall mass was biopsied. The patient was transferred to DHMC. Physical examination here detected additional adenopathy at the angle of the jaw. Labs WBC 9300, Hgb 12.7gr., Platelets 288K, BUN 10, LDH 664, other LFT’s normal.
J.C. Diagnosis: Burkitt Lymphoma • Bone marrow negative for lymphoma • CSF positive for Burkitt lymphoma • Treatment • Prognosis • Current status
Burkitt lymphoma-lessons • 2% of all lymphomas in adults • 1/3 of all lymphomas in children • Increased incidence in HIV disease • Very aggressive B cell lymphoma • Can present as acute leukemia or with leukemic component • Pathogenesis: Translocations bringing the myc cell cycle control gene/oncogene normally on chromosome 8 to sites of constitutively expressed B cell antigen receptor genes/ promoters • Results in excessive myc production and constant replication • T(8;14) Ig heavy chain gene • T(2;8) Ig kappa light chain gene • T(8;22) Ig lambda light chain gene
Burkitt lymphoma • In Africa, associated with Epstein-Barr virus (endemic Burkitt’s) • Not so in US (non-endemic Burkitt) • In US, usually presents in abdomen, often with acute abdomen/bowel obstruction • Until 10 years ago, rapid fatal, with median survival <1year • Now cure rates >80% in children, 40-50% in adults (less in HIV setting) • Requires very aggressive, multiagent therapy
Pt. O.I.- Clinical presentation • O.I. was a 61 y.o. male in April, 1997 when he noted the onset of discomfort in his right groin and testicle with walking, accompanied by a small nodule in his right groin. A CT scan of the abdomen and pelvis revealed a right retroperitoneal mass extending into the pelvis. A needle biopsy of the retroperitoneal mass was performed at an outside hospital, which led to a diagnosis of undifferentiated neoplasm suspicious for large cell lymphoma. A week later, the patient was transferred to DHMC for further evaluation and treatment. In the interim period, the mass demonstrated rapid enlargement, with an LDH level rising from 1200 to 7000U. A repeat needle biopsy and aspirate were performed at DHMC for further characterization of the tumor. Sufficient cells were obtained to perform flow cytometric analysis. Material for cytogenetics was also submitted.