Download
1 / 70
830 likes | 1.33k Views
The Digestive Tract. The GI tract (gastrointestinal tract) The muscular alimentary canal Mouth Pharynx Esophagus Stomach Small intestine Large intestine Anus The accessory digestive organs Supply secretions contributing to the breakdown of food Teeth & tongue Salivary glands

E N D
The GI tract(gastrointestinal tract) The muscular alimentary canal • Mouth • Pharynx • Esophagus • Stomach • Small intestine • Large intestine • Anus • The accessory digestive organs Supply secretions contributing to the breakdown of food • Teeth & tongue • Salivary glands • Gallbladder • Liver • Pancreas
The Digestive Process • Ingestion • Taking in food through the mouth • Propulsion (movement of food) • Swallowing • Peristalsis – propulsion by alternate contraction &relaxation • Mechanical digestion • Chewing • Churning in stomach • Mixing by segmentation • Chemical digestion • By secreted enzymes: see later • Absorption • Transport of digested end products into blood and lymph in wall of canal • Defecation • Elimination of indigestible substances from body as feces
Chemical digestion • Complex food molecules (carbohydrates, proteins and lipids) broken down into chemical building blocks (simple sugars, amino acids, and fatty acids and glycerol) • Carried out by enzymes secreted by digestive glands into lumen of the alimentary canal
Ways to divide…. The more common Plus: epigastric periumbilical suprapubic flank
Histology of alimentary canal wallSame four layers from esophagus to anal canal • Mucosa • Submucosa • Muscularis externa • Serosa from lumen (inside) out
Inner layer: the mucosa*(mucous membrane) Three sub-layers • Lining epithelium • Lamina propria • Muscularis mucosae *
More about the mucosa • Epithelium: absorbs nutrients, secretes mucus • Continuous with ducts and secretory cells of intrinsic digestive glands (those within the wall) • Extrinsic (accessory) glands: the larger ones such as liver and pancreas • Lamina propria • Loose connective tissue with nourishing and absorbing capillaries • Contains most of mucosa-associated lymphoid tissue (MALT) • Muscularis mucosae • Thin layer of muscle producing only local movements
Second layer: the submucosa* • Connective tissue containing major blood and lymphatic vessels and nerves • Many elastic fibers so gut can regain shape after food passes *
Next in, the muscularis externa*(AKA just “muscularis”) Two layers of smooth muscle responsible for peristalsis and segmentation • Inner circular layer (circumferential) • Squeezes • In some places forms sphincters (act as valves) • Outer longitudinal layer: shortens gut *
Last (outer), the serosa*(the visceral peritoneum) • Simple squamous epithelium (mesothelium) • Thin layer of areolar connective tissue underneath • Exceptions: • Parts not in peritoneal cavity have adventitia, lack serosa • Some have both, e.g. retroperitoneal organs *
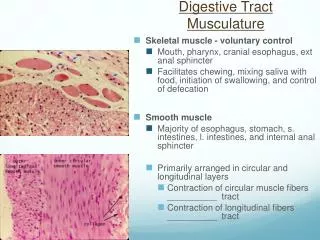
Smooth muscle Smooth muscle • Muscles are spindle-shaped cells • One central nucleus • Grouped into sheets: often running perpendicular to each other • Peristalsis • No striations (no sarcomeres) • Contractions are slow, sustained and resistant to fatigue • Does not always require a nervous signal: can be stimulated by stretching or hormones • 6 major locations: • inside the eye 2. walls of vessels 3. respiratory tubes • 4. digestive tubes 5. urinary organs 6. reproductive organs
Nerves • Enteric nervous system: the gut’s own • Visceral plexuses within gut wall controlling the muscles, glands and having sensory info • Myenteric: in muscularis • Submucosal • 100 million neurons! (as many as the spinal cord) • Autonomic input: speeds or slows the system • Parasympathetic • Stimulates digestive functions • Sympathetic • Inhibits digestion • Largely automatic
Review of some definitions…. • Peritoneum: serous membranes of the abdominopelvic cavity • Visceral peritoneum: covers external surfaces of most digestive organs • Parietal peritoneum: lines body wall • Peritoneal cavity: slit-like potential space between visceral and parietal peritoneum • Serous fluid – lubricating
New definitions • Mesentery • Double layer of peritoneum • Extends to digestive organs from body wall • Hold organs in place • Sites of fat storage • Route by which circulatory vessels and nerves reach organs • Most are dorsal • Extend dorsally from gut to posterior abdominal wall • Ventral mesentery – from stomach and liver to anterior abdominal wall • Some mesenteries are called “ligaments” though not technically such
Mesenteries • Note dorsal, ventral and formation of retroperitoneal position
Mesenteries • Two ventral mesenteries • Falciform “ligament” • Binds anterior aspect of liver to anterior abdominal wall and diaphragm • Lesser omentum (=“fatty skin”) – see diagram* • All other mesenteries are dorsal (posterior) *
Mesenteries continued (all these are dorsal) • Greater omentum • Connects stomach to posterior abdominal wall – very roundabout • Wraps around spleen: gastrosplenic ligament • Continues dorsally as splenorenal ligament • A lot of fat • Limits spread of infection by wrapping around inflamed e.g. appendix • “Mesentery” or mesentery proper • Supports long coils of jejunum and ileum (parts of small intestine) • Transverse mesocolon • Transverse colon held to posterior abdominal wall • Nearly horizontal sheet fused to underside of greater omentum • Sigmoid mesocolon • Connects sigmoid colon to posterior abdominal wall see next slides for pics…
Note mesenteries: falciform ligament, lesser omentum, greater omentum
Note: greater omentum, lesser omentum, falciform ligament, transverse mesocolon, mesentery, sigmoid mesocolon
Some organs are “retroperitoneal” • Are “behind the peritoneum” • Fused to posterior (dorsal) abdominal wall • Lack a mesentery • Include: • Most of duodenum (1st part of small intestine) • Ascending colon • Descending colon • Rectum • Pancreas • Tend to cause back pain, instead of abdominal pain (This is as opposed to the organs which are intraperitoneal, or just “peritoneal”)
The Mouth • Mouth = oral cavity • Lining: thick stratified squamous epithelium • Lips- orbicularis oris muscle • Cheeks – buccinator muscle
“Vermillion border” or red border • Between highly keratinized skin of face and mucosa of mouth • Needs moisture • Note frenulums (folds of mucosa) • Palate – roof of mouth • Hard plate anteriorly • Soft palate posterioly • Uvula
Tongue • Mostly muscles • Grip and reposition food • Forms “bolus” of food (lump) • Help in swallowing • Speech – help form some consonants • Note frenulum on previous slide: can be too tight • Taste buds contained by circumvallate and fungiform papillae • Lingual tonsil – back of tongue
Teeth • Called “dentition” (like dentist) • Teeth live in sockets (alveoli) in the gum-covered margins of the mandible and maxilla • Chewing: raising and lowering the mandible and moving it from side to side while tongue positions food between teeth
Teeth • Two sets • Primary or deciduous • “Baby” teeth • Start at 6 months • 20 are out by about 2 years • Fall out between 2-6 years • Permanent: 32 total • All but 3rd set of molars by end of adolescence • 3rd set = “wisdom teeth” • Variable • Some can be “impacted” (imbedded in bone)
Teeth are classified according to shape and function • Incisors: chisel-shaped for chopping off pieces • Canines: cone shaped to tear and pierce • Premolars (bicuspids) and • Molars - broad crowns with 4-5 rounded cusps for grinding incisor canine premolar molar Cusps are surface bumps
Tooth structure • Two main regions • Crown (exposed) • Root (in socket) • Meet at neck • Enamel • 99% calcium crystals • Hardest substance in body • Dentin – bulk of the tooth (bone-like but harder than bone, with collagen and mineral) • Pulp cavity with vessels and nerves • Root canal: the part of the pulp in the root A C B
Tooth structure • Cementum – bone layer of tooth root • Attaches tooth to periodontal ligament • Periodontal ligament • Anchors tooth in boney socket of the jaw • Continuous with gingiva (gums) • Cavities or caries - rot • Plaque – film of sugar, bacteria and debris A C B
Salivary glands(tuboalveolar glands) • Intrinsic salivary glands – within mucosa • Secrete saliva all the time to keep mouth moist • Extrinsic salivary glands • Paired (2 each) • Parotid • Submandibular • Sublingual • External to mouth • Ducts to mouth • Secrete saliva only right before or during eating Saliva: mixture of water, ions, mucus, enzymes keep mouth moist dissolves food so can be tasted moistens food starts enzymatic digestion buffers acid antibacterial and antiviral
Extrinsic salivary glands • Parotids* - largest (think mumps) • Facial nerve branch at risk during surgery here • Submandibular # - medial surface mandible • Sublingual + - under tongue; floor of mouth * + Compound = duct branches Tubo = tubes Alveolar = sacs #
Pharynx ___oropharynx • Oropharynx and laryngopharynx • Stratified squamous epithelium • Three constrictor muscles* • Sequentially squeeze bolus of food into esophagus • Are skeletal muscles • Voluntary action • Vagus nerve (X) ___laryngopharynx * * *
Esophagus • Continuation of pharynx in mid neck • Muscular tube collapsed when lumen empty • Descends through thorax • On anterior surface of vertebral column • Behind (posterior to) trachea Esophagus___________ *
Esophagus continued • Passes through “esophageal hiatus” in the diaphragm to enter the abdomen • Abdominal part only 2 cm long • Joins stomach at cardiac orifice* • Cardiac sphincter at cardiac orifice to prevent regurgitation (food coming back up into esophagus) • Gastroesophageal junction and GERD ___________________esophageal hiatus (hiatus means opening) *
Microscopic anatomy of esophagus Contains all 4 layers (see right) • Epithelium: nonkeratinized stratified squamous epithelium • At GE junction – thin simple columnar epithelium • Mucus glands in wall • Muscle (muscularis externa) changes as it goes down • Superior 1/3 of esophagus: skeletal muscle (like pharynx) • Middle 1/3 mixture of skeletal and smooth muscle • Inferior 1/3 smooth muscle (as in stomach and intestines) • When empty, mucosa and submucosa lie in longitudinal folds
Stomach • J-shaped; widest part of alimentary canal • Temporary storage and mixing – 4 hours • Into “chyme” • Starts food breakdown • Pepsin (protein-digesting enzyme needing acid environment) • HCl (hydrochloric acid) helps kill bacteria • Stomach tolerates high acid content but esophagus doesn’t – why it hurts so much when stomach contents refluxes into esophagus (heartburn; GERD) • Most nutrients wait until get to small intestine to be absorbed; exceptions are: • Water, electrolytes, some drugs like aspirin and alcohol (absorbed through stomach)
Stomach epigastrium • Lies mostly in LUQ • But pain can be epigastric or lower • Just inferior to (below) diaphragm • Anterior (in front of) spleen and pancreas • Tucked under left lower margin of liver • Anchored at both ends but mobile in between • Main regions in drawing to right-------------------------------- • Capacity: 1.5 L food; max capacity 4L (1 gallon) dome junction with esophagus contains pyloric sphincter funnel shaped
Stomach Regions • Cardiac region • Fundus (dome shaped) • Body • Greater curvature • Lesser curvature • Pyloric region • Antrum • Canal • Sphincter dome junction with esophagus contains pyloric sphincter funnel shaped
Rugae: longitudinal folds on internal surface (helps distensibility) • Muscularis: additional innermost oblique layer (along with circular and longitudinal layers)
Histology of stomach • Simple columnar epithelium: secrete bicarbonate-buffered mucus • Gastric pits opening into gastric glands • Mucus neck cells • Parietal cells • HCL • Intrinsic factor (for B12 absorption) • Chief cells • Pepsinogen (activated to pepsin with HCL) • Stimulated by gastrin: a stomach hormone
Small intestine • Longest part of alimentary canal (2.7-5 m) • Most enzymatic digestion occurs here • Most enzymes secreted by pancreas, not small intestine • Almost all absorption of nutrients • 3-6 hour process • Runs from pyloric sphincter to RLQ Small intestine___________
Blood supply: superior mesenteric artery; Veins drain into hepatic portal vein • Small intestine has 3 subdivisions • Duodenum – 5% of length • Jejunum – almost 40% • Ileum – almost 60% Duodenum is retroperitoneal (stuck down under peritoneum); others are loose Duodenum receives bile from liver and gallbladder via bile duct* enzymes from pancreas via main pancreatic duct* * *
Small intestine designed for absorption • Huge surface area because of great length • Structural modifications also increase absorptive area • Circular folds (plicae circulares) • Villi (fingerlike projections) 1 mm high – simple columnar epithelium: velvety • Microvilli Absorptivie cell with microvilli to increase surface area & many mitochondria: nutrient uptake is energy-demanding * Lacteal*: network of blood and lymph capillaries -Carbs and proteins into blood to liver via hepatic portal vein -Fat into lymph: fat-soluble toxins e.g. pesticides circulate systemically before going to liver for detoxification
Intestinal crypts* (of Lieberkuhn) inbetween villi • Cells here divide every 3-6 days to renew epithelium (most rapidly dividing cells of the body) • Secrete watery intestinal juice which mixes with chyme (the paste that food becomes after stomach churns it) • Intestinal flora – the permanent normal bacteria • Manufacture some vitamins, e.g. K, which get absorbed -have many mitochondria: nutrient uptake is energy-demanding Duodenal glands* * • Mucus to counteract acidity from stomach • Hormones: • Cholecystokinin (stimulates GB to release stored bile, also pancreas) • Secretin (stimulates pancreatic ducts to release acid neutralizer) * -produce mucus
Large intestine Digested residue reaches it Main function: to absorb water and electrolytes Subdivisions Cecum Appendix Colon Rectum Anal canal