Download
1 / 17
170 likes | 242 Views
What a family doctor and pediatrician should do at diagnosis. Mason Bond Nov 2003. Pediatric Oncology. Only 1-2/10,000 children/ year in US are diagnosed with cancer In British Columbia about 130 children are diagnosed with cancer each year Index of suspicion

E N D
What a family doctor and pediatrician should do at diagnosis Mason Bond Nov 2003
Pediatric Oncology • Only 1-2/10,000 children/ year in US are diagnosed with cancer • In British Columbia about 130 children are diagnosed with cancer each year • Index of suspicion • Overall the prognosis for cure is quite good
Pediatric Oncology • Discuss / refer patients suspected of having a malignancy • Referral to surgical services at BC Children’s may also be appropriate • On-call service (604)875-2161 • Written communication alone is not usually adequate
Pediatric OncologyCytopenias • Isolated neutropenia is common and usually benign • Repeat in a week • Multiple cell lines affected with or without organomegaly/ lymphadenopathy • Consider leukemia • Chest X-ray, uric acid, LDH • Warrants discussion or consultation
Pediatric OncologyLymphadenopathy • Common problem • Majority infections/ post-infectious • Non Hodgkin’s Lymphoma with generalized adenopathy: lymphoblastic or ALL • screen: • CBC, uric acid, LDH
Pediatric OncologyLymphadenopathy • Single node • Still commonly infection • Recall Hodgkin’s uncommon <10 years and rare < 5 years • NHL- lymphoblastic, large cell, Burkitts • Assure no other findings • Screen and watch versus referral • Definitely refer if consider biopsy
Pediatric OncologyWhat to do at diagnosis • Assure safety of patient • Investigations related to patient safety are always appropriate • Medical status should always be discussed prior to transfer
Pediatric OncologySafety considerations • Leukemia • Infection and bleeding • Tumor lysis • Mediastinal mass • Leukostasis • Solid tumor • Mechanical • Lymphoma and tumor lysis
Pediatric Oncology • Definitive diagnostic procedure should be done at B.C. Children’s • Cytogenetic, immunocytology in leukemia • Advances in molecular pathology • Impact of surgical biopsy on local therapy options and prognosis
COG Low Risk ALL Must have all of the following: • NCI standard risk for induction • Have either: • Trisomies 4, 10, 17 (all three) OR • TEL/AML-1 • RER (M1 day 15) • No adverse translocations: • E2A-PBX-1, MLL, BCR/ABL • No CNS-3/2 or testicular involvement
Standard Risk ALL Must have: • NCI Standard Risk Must not have: • MLL or BCR-ABL • <45 chromosomes or DI <0.81 • SER or MRD (day 28) >0.1%, unless has trisomies 4, 10, 17 or TEL/AML1
High Risk Group COG ALL – B-precursor Must have one or more: • NCI High Risk • NCI Standard Risk if SER or MRD (day 28) >0.1% • MLL rearrangement Must not have: • BCR-ABL • <45 chromosomes or DI <0.81 • Failed induction
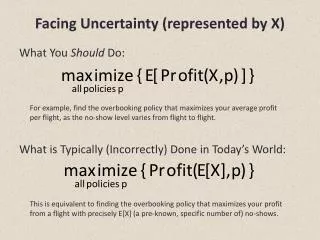
Outcome by New COG R.G. Definitions 1.0 Low Risk (n=162) Standard Risk (n=503) High Risk (n=445) 0.8 0.6 Very High Risk (n=49) Probability 0.4 2 Yr Risk GroupEFS (%)SE (%) Low 98.4 1.2 Standard 94.4 1.3 High 90.1 2.0 Very High 59.4 12.0 CCG 1950/60s Series B-precursor ALL 0.2 0.0 0 1 2 3 4 5 Years Followed 7/2001
Pediatric Oncology • Fresh and frozen tissue needed for molecular pathology • Rhabdomyosarcoma alveolar t(2;13) and t(1;13) PAX3 and PAX7/FKHR • Ewing’s family tumors t(11;22) EWS-FLI1 • Desmoplastic small round cell t(11;22) EWS-WT1 • Synovial cell sarcoma t(X;18)
Pediatric Oncology • Pathology and prognosis • N-myc amplification in neuroblastoma • t(1;13) vs t(2;13 in metastatic alveolar RMS • Surgery and prognosis • Close margin versus wide resection • Biopsy site and local control
Pediatric Oncology • Provide information to family • Why refer • Possible length of stay • What your role will be later • Send information with family • Lab results • radiology
Pediatric Oncology • Diagnosis of cancer considered/ suspected • Discuss/ referral • Assure safety • Family information/ support • www.cw.bc.ca/ch_oncology