Download
1 / 16
170 likes | 357 Views
Management of DCIS. KWH Experience. Dr. Carmen Ho. Ductal carcinoma in situ (DCIS ). Breast cancer as most common cancer in women in Hong Kong DCIS as precursor of invasive cancer Heterogeneous group with diverse malignant potential Incidence of DCIS increased with mammographic screening

E N D
Management of DCIS KWH Experience Dr. Carmen Ho
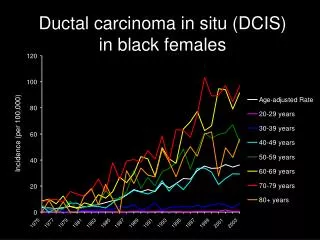
Ductal carcinoma in situ (DCIS) • Breast cancer as most common cancer in women in Hong Kong • DCIS as precursor of invasive cancer • Heterogeneous group with diverse malignant potential • Incidence of DCIS increased with mammographic screening • 3/100,000 to 34/100,000 in 50-69 years old Steenbergen. Breast Cancer Res Treat.2009. • Best treatment for DCIS remains a controversy
Management of DCIS • Mastectomy vs. breast conserving treatment + RT • RT reduces local recurrence rate (13.4% vs. 3.9%) NSABP B-17 • Similar local recurrence and survival NSABP B-04 • Acceptance of BCT in Chinese (survey) • 29-49% Chua et al. Breast J. 2005 • BCT rate in HK for breast cancer : 22-30% Yau et al. Int J Radiat Oncol Biol Phys. 2008
KWH experience in DCIS • Retrospective study • Period : January 2002 – April 2009 • Inclusion • Patients diagnosed with DCIS after surgical excision • Patients with micro- or invasive features were not included • 212 patients included • Age : 57.2 (37.8 – 87.5) • Median FU : 31.0 months (0.3 - 81.4 months) • Bilateral disease : 22 • 7 with bilateral disease on presentation
PREsentations • Average size : 2.02cm (0.1 – 7 cm) • Size • Screen detected group : 1.32cm • Symptomatic group : 2.47cm (P<0.01)
Treatment • BCT offered to 175 patients • Unicentric tumor <3cm • Appropriate tumor to breast ratio • Acceptance of adjuvant radiotherapy • 104 patients accepted BCT (59.4%) • 75% were screen detected
Adjuvant Radiotherapy • 96.2% (100/104) have adjuvant RT • 4 patients with small foci (<0.6cm) and low grade DCIS • 1 has IBTR 5 years later as DCIS
OUTcome • 32 patients (31.7%) receiving BCT have close margin (<3mm) • 5 patients underwent re-excision • 8 required subsequent mastectomy • Boost dose of radiotherapy • All free of local recurrence • Sentinel LN biopsy was done in 98 patients • Positive sentinel LN noted in 3 patients • Axillary dissection was performed
Disease free • 198 / 212 (93.4%) remained disease free • Screen detected : 95.4% (124/130) • Symptomatic : 90.2% (74/82)
Local recurrence • 4 patients with BCT have ipsilateral breast tumor recurrence (3.8%) • 3 recurred as invasive ductal carcinoma, subsequent mastectomy performed • 1 recurred as DCIS with ROLL done • All remained disease free after salvage treatment
Disease related mortality • 1 patient died • Presented with blood stained nipple discharge • Microdochectomy performed : DCIS with involved margin • Simple mastectomy performed • DCIS (high grade with comedo necrosis) • 6 months after mastectomy, developed bone metastasis
Discussion • Emphasize on importance of screening mammogram • Acceptance of BCT + RT as treatment • 75% patients receiving BCT were screen detected • 69% with clear margin (>3mm) • Positive sentinel LN in 3.0% patients with DCIS • Risk of local recurrence after BCT 3.8% with median FU 31.0 months • Success of salvage treatment after IBTR