Download
1 / 48
861 likes | 1.99k Views
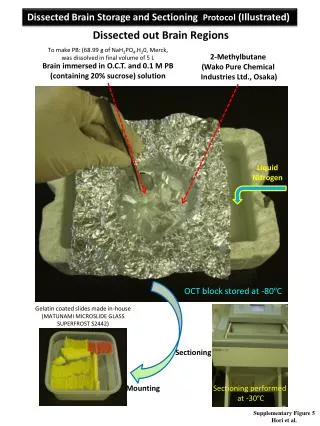
The Production of Health Folland et al chaps 5. Outline. Aim: Understand how health is produced The Production Function of Health The Historical Role of Medicine and Health Care The Production Function of Health in the Modern Day How Does Health Care Affect Other Measures of Health?

E N D
The Production of Health Folland et al chaps 5
Outline Aim: Understand how health is produced • The Production Function of Health • The Historical Role of Medicine and Health Care • The Production Function of Health in the Modern Day • How Does Health Care Affect Other Measures of Health? • The Role of Schooling • Conclusions
Health status • How do we measure health? • What are the inputs that produce health? • How do we evaluate their productivity?
The measurement of health What are the possible measures for health? • The most popular in the literature is mortality. • Mortality rates: Deaths per period/individuals alive at the beginning of the period. • Infant mortality rate: Deaths in the first year of life/births • Neonatal mortality: deaths in the first 28 days • Life expectancy at birth • What are the limits of it? • Other possibilities include: morbidity (illness) rates and disability days.
The production function of health Production function: How the level of output depends on quantities of various inputs The production function of health defines the relationship between health inputs and healthstatus over a specified time period. What are the inputs that produce health status (HS)? • In general: HS = HS (Health care, Lifestyle, Environment, Human Biology)
Total Product Health status increases as more and more health care inputs are added to the production process. Inputs and outputs are measured over an implied period such a year. Figure 5-1 A Production of Health
Variables of the health production function Health status: level of health at a point in time Health care: quantity of medical care consumed Lifestyle: composite, multidimensional factor including the individual’s habits, household structure, physical and social environments, occupation, devotion to career, composition of consumption, level and type of exercise and recreational and spiritual activities Environment: a variety of environmental factors, including air and water quality • How does the production curve move if a more efficient treatment for cancer is introduced?
The production function The production function in Fig. 1A is a raising curve that flattens out at higher levels of health care but never bends downward. Would the health production eventually bend downward? In other words: Is it possible to get too much health care so that the health of the population is harmed? Yes! Iatrogenic (meaning provider-caused) disease is an inevitable by-product of many medical interventions. Examples: • each surgery has its risk; • combinations of drugs may have unforeseen and adverse interactions.
Marginal product The marginal contribution of health care is its marginal product, meaning the increment to health caused by one extra unit of Health Care, coeterisparibus (holding all other inputs constant). Increasing Health Care from 0 to 1 unit in Fig. 1A improves health status by ∆HS1, the first unit’s marginal product.
Marginal product (cont.) Law of diminishing marginal returns: marginal products are diminishing in size. If society employs a total of n units of Health Care, then the total contribution of Health Care is the sum of the marginal products of each of the n units. The total contribution (AB in Fig. 1A) may be substantial, while the marginal product of the nth unit of medical care is ∆HSn and it is small (we are nearly on the “flat of the curve”).
Marginal Product Diminishing marginal product – as more and more health care inputs are added to the production process, the increments in heath status diminish. Figure 5-1B Production of Health
Marginal Product and Health Care Policy Often, the marginals, rather than the totals, are relevant to policy propositions. For example, no one seriously recommends that society eliminates all health care spending. However, it is reasonable to ask whether society would be better off if it could reduce health care expenditures by $1 billion and invest those funds in another productive use, such as housing, education, transportation, defense, or other consumption.
The historical role of medicine and health care: An overview • Many medical historians agree that practitioner-provided medical interventions played only a small, perhaps negligible, role in the historical decline in population mortality rates. • A larger role, one of the most significant ones, might be attributed to public health measures and the spread of knowledge of the sources of disease. • A number of scholars in this field attribute the largest share of the credit to improvements in environment, particularly to the greatly increased supply of foodstuffs that became available due to the agricultural and industrial revolutions.
Rising Population and the Role of Medicine Figure 5-2 World Population from 10,000 BCE to Modern Day Source: http://www.ciese.org/curriculum/popgrowthproj/worldpop.html. Data from U.S. Census Bureau.
Rising Population and the Role of Medicine (cont.) Population increase comes from: • increased birth rates (fertility); • reduced mortality; • increased net in-migration. Thomas McKeown (1976) studied the population dynamic in England and Wales (1841-1071). • birth rates have declined (common finding in countries undergoing industrialization and modernization) • mortality rates did decline substantially; • migration was not an important source of population increase.
What caused the mortality rate declines? Was it medicine? McKeown investigated which diseases contributed to the decline in death rates for three time periods. Table 5-1 Death Rates (per million) in 1848-1854, 1901, and 1907
What caused the mortality rate declines? Was it medicine? (cont.) • Was the decline in mortality rates due to improvements in medical science provided to the public through medical practice? In most cases, an effective specific medical intervention was not available until late in the period, well after the great part of the mortality had occurred.
What caused the mortality rate declines? Was it medicine? (cont.) Example: • Airborne infectious diseases account for the largest single portion of mortality reduction (in particular, bronchitis, pneumonia, and influenza). The availability of effective medical intervention for these diseases started after 1930!
Did Medicine Cause the Decline in Mortality Rates? Figure 5-3. Fall in the Standardized Death Rate per 1,000 Population for Four Common Infectious Diseases in Relation to Specific Medical Measures for the United States Source: Reprinted from Milbank Memorial Fund Quarterly/Health and Society, John B. Mckinlay and Sonja M. Mckinlay, “The Questionable Contribution of Medical Measures to the Decline of Mortality in the United States in the Twentieth Century, Milbank Memorial Fund Quarterly/Health and Society 55 (1977): 405–428, with the permission of Blackwell Publishers.
Nutrition Reduced Mortality Medical historian Thomas McKeown (1976) and economic historian Robert Fogel (2004), argued strongly that the main cause of decreasing mortality was improved nutrition.
Public Health Reduced Mortality Public health advocates claim that public health, which began about 1850 enormously contributed to reduce mortality. Example: The transition from water tainted with infectious organisms to clean water supplies was the most dramatic change in the health environment of city dwellers.
What Lessons Are Learned from the Medical Historian? • We cannot conclude that medical research is unimportant in history or in the present day. • Medical research contributes not only through improvements to medical practice, but also through its influence on health-enhancing practices. • Example: typhoid declined substantially well before the arrival by 1950 of chloramphenicol. Medical research, however, contributed to our understanding of the cause and transmission of typhoid and generated public health measures such as filtering public water supplies, chlorination of water supplies and establishment of drinking-water standards. • Selma Mushkin (1979) estimates that medical research accounted for almost one-third of the cost savings to society from reduction in sickness or death rates in the US from 1900 to 1975.
The production of health in the modern day. Preliminary Issues • Challenges with the measurement of health. We desire a measure of population health status that • captures the aspects of health status that are meaningful • and that we can measure with adequate precision. Mortality rates are accurate but do not capture several meaningful aspects of health status such as: • reduction in pain and suffering • and other improvements in the quality of life • Analysts have used other indicators of health status: • morbidity (illness) rates • and disability days
The contribution of health care to population health: some empirical evidence We look at the elasticity of health output with respect to health care expenditurein some empirical studies. Table 5-2 Measuring the Contribution of Health Care to Population Health
Is Health Care Worth It? • We have found that health care is a statistically significant contributor to health on the margin, but that its marginal effect on health is small. Research suggests that the elasticity of health care at the margin is 0.10.
Is Health Care Worth It? An example To illustrate the meaning of this elasticity, suppose that the Congress reallocate $250 billion from other programs to health care expenditure. The year before the US spent $2.5 trillion on health care The $250 billion transfer would increase health care expenditure by 10% improvement in health is 10*0.10=1%. If we define “health” by average life expectancy, a 1% gain would mean an increased average life expectancy of 78*0.01=0.78 year (about 9.4 months). Spread over population the 0.78 year of life could lead to benefits that exceed costs.
Prenatal care The importance of examining population subgroups comes from neonate mortality studies. Neonate: infant one month old or younger Neonatal mortality rate: deaths to neonates per 1,000 live births. How can we reduce these deaths?
Contribution of selected factors to reductions in neonate mortality: some empirical evidence Table 5-3 Contribution of Selected Factors to Reductions in Neonate Mortality Rates, 1964-1977
Contribution of selected factors to reductions in neonate mortality: some empirical evidence (cont.) WIC: governmental program designed to provide improved nutrition for poor women, infants and children. BCHS: author’s measure combining various Bureau of Community Health Services projects, including maternal and infant care, as well as community health centers. EC386 Carmen A. Li
Contribution of selected factors to reductions in neonate mortality: some empirical evidence (cont.) • Blacks benefit more from health care on the margin. • The WIC program reduced: • white neonate mortality rates of 0.425 deaths per 1,000 live births • black neonate mortality by 1.33 deaths per 1,000 live births. • Abortion lower mortality. This result may reflect that many abortions were of fetuses that would not have survived infancy • Prenatal care is effective (especially for blacks)
The World’s Pharmacies Recent research (Shaw, Horrace, and Vogel, 2005; Miller and Frech, 2004) finds that Organization for Economic Cooperation and Development (OECD) countries with higher drug consumption have greater life expectancies. The magnitude of the effect is on a par with the effects of reduced cigarette consumption and increases of fruit and vegetables in the diet.
How does health care affect other measures of health? Mortality rates tell only part of the health care story, other measures of health also should be examined. These include morbidity data and other indicators of health. Work also is being done on developing a measure of the quality of life, and quality of life may become the subject of production studies.
How does health care affect other measures of health?: the RAND Health Insurance Experiment • The RAND Health Insurance Experiment (RAND HIE) was a large-scale, randomized experiment of health care costs, utilization and outcomes in the United States which assigned people randomly to different kinds of plans and followed their behavior between 1971 and 1982. • For the study, RAND recruited 2,750 families encompassing more than 7,700 individuals, all of whom were under the age of 65. EC386 Carmen A. Li
How does health care affect other measures of health?: the RAND Health Insurance Experiment (cont.) The RAND Health Insurance Experiment (RHIE) was designed to test the effect of alternative health insurance policies on • the demand for health care; • the health status of a large and closely observed group of people. Findings: • the greater the portion that individuals are required to pay, the less health care they choose to purchase; • no health differences were found between the groups studied
How does health care affect other measures of health?: the RAND Health Insurance Experiment (cont.) RAND subjects are divided into 4 groups, which differ by type of health insurance policy: • subjects who pay nothing out of their pocket for their health care • subjects who pay 25 to 50 % of their bill themselves; • Subject who pay all of their health care bills up to a certain amount, called deductible at individual level; • Subject who pay all of their health care bills up to a certain amount, called deductible at family level. The subject’s out of the pocket cost ranges from zero (free) to about 95% of the bill.
How does health care affect other measures of health?: the RAND Health Insurance Experiment (cont.) The results showed that cost sharing reduced the use of nearly all health services.
How does health care affect other measures of health?: the RAND Health Insurance Experiment (cont.) Table 5-4 Work Loss Days per Employed Person per Year, by Plan Work loss days per employed per year: a measure of health status that ties directly to both health and productivity. Newhouse et al. (1993) : “Our results show that the 40 percent increase in services on the free-care plan had little or no effect on health status for the average adult.”
How does health care affect other measures of health?: the RAND Health Insurance Experiment (cont.) Implication: it seems from the RAND results that public provision of health insurance might not be justifiable on the basis of benefits to health. BUT… J. Gruber (2008): no one in the RAND experiment was completely without insurance! The least insured individual studied by RAND had full coverage for health expenditure above a deductible, that was $1000. Later studies of the truly uninsured show significant health gains from the provision of public insurance (Currie and Gruber, 1996; Doyle, 2005; Hanratty, 1996). These studies report reductions in infant and neonate deaths of around 5 to 10%.
The Importance of Lifestyle and Environment Victor Fuchs studied the death rates in two contiguous states, Nevada and Utah, that are similar in many ways: levels of income and medical care and are alike in many other aspects. Table 5-5 Excess of Death Rates in Nevada Compared with Utah, Average for 1959-1961 and 1966-1968
The Importance of Lifestyle and Environment • Average death rates in Nevada were greater than those in Utah. • Fuchs argued that the explanation for these substantial differences surely lies in lifestyle and environment: “Utah was, and remains, inhabited primarily by Mormons, whose influence is strong throughout the state. Devout Mormons do not use tobacco or alcohol and in general lead stable, quiet lives. Nevada, on the other hand, is a state with high rates of cigarette and alcohol consumption and very high indexes of marital and geographical instability.”
Cigarettes, Exercise and a Good Night’s Sleep • Smoking and other lifestyle behavior can be determined by unobserved variables that affect health status. • Recent research (Balia and Jones, 2008; Contoyannis and Jones, 2004) addresses this problem in studying human behavior by estimating both the determinants of lifestyle behaviors as well as the determinants of health status, giving a clearer picture of the importance of lifestyle. • The authors showed that a good night’s sleep, avoiding smoking, and regular exercise each contribute importantly to self-reported health.
The Family as Producer of Health In understanding health impacts it may be valuable to view the family as a producer of health. Research (Rosenzweig and Schultz, 1983; Rosenzweig and Wolpin, 1995; Joyce, Racine, and Mocan, 1992) suggests that maternal lifestyle issues, like, smoking and drug use can negatively impact the production of newborn health. Evans and Ringel (1999) find that taxing cigarettes leads to improved birth outcome via its effect on smoking behaviors of expectant mothers.
Social Capital and Health Social capital (= the networks of social contacts of an individual like family, friends and the community) may improve health in several ways: • it may relieve stress to have the support of more social contacts; • more contacts can provide additional information on healthful behaviors and health purchases; • satisfying social relationships may provide reasons to re-evaluate risky health behaviors. • Challenge: how to determine whether social capital causes better health or whether it is a result of some other factors
Environmental Pollution • Pollution effects on health are sizable and statistically significant in both industrialized and lesser-developed countries (Cropper et al., 1997). • The degree to which reductions in pollution will improve the health of populations is less clear.
Income and Health • Pritchett and Summers (1996) leave little doubt that extremely low incomes have a strong effect on people’s health.
The Role of Schooling • Education makes people more efficient producers of their own health (Grossman, 1972a, 1972b; Lleras-Muney, 2005). • By 1960 education appeared to have increased life years by 1.7 years.