Download
1 / 33
360 likes | 616 Views
Stressors Affecting Elimination Urinary. NUR101 Fall 2008 Lecture # 22 K. Burger, MSED, MSN, RN, CNE PPP By Sharon Niggemeier RN, MSN. Anatomy & Physiology. Kidneys Ureters Bladder Urethra http://www.youtube.com/watch?v=glu0dzK4dbU&feature=related. Anatomy & Physiology MATCHING.

E N D
Stressors Affecting EliminationUrinary NUR101 Fall 2008 Lecture # 22 K. Burger, MSED, MSN, RN, CNE PPP By Sharon Niggemeier RN, MSN
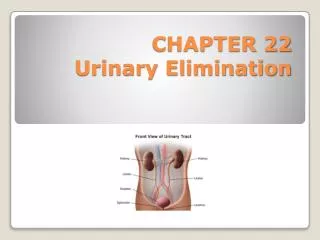
Anatomy & Physiology • Kidneys • Ureters • Bladder • Urethra • http://www.youtube.com/watch?v=glu0dzK4dbU&feature=related
Anatomy & PhysiologyMATCHING • Let’s test our ?PRIOR? Knowledge of the renal system. • http://www.freenursetutor.com/urinary/flashcards-matching-urinary-system.html
Nephron Function • Functional unit of kidney • 1 million per kidney • 1200 ml blood pass through the kidney/min • Wastes cannot be excreted as solids; must be excreted in solution • Normal urine production = 1 ml / minute • Kidneys must produce 30 ml/hr minimum
Critical Thinking • A client in hemorrhagic shock may proceed quickly into concomitant renal failure. Why? Glomerular capillary blood pressure is the driving force of glomerular filtration. If blood pressure is not maintained, there is not enough osmotic gradient to sustain filtration.
Nephron Function • Blood filtered through glomerulus • this filtrate moves into Bowman’s capsules • proceeds into proximal tubule where water /electrolytes/glucose & protein are reabsorbed • Loop of Henley – water andsolutes such as Na & Cl, are reabsorbed (urine becomes more concentrated) • distal convoluted tubules allows for water and NA reabsorbtion. Controlled reabsorption (by ADH antidiuretic hormone) regulates F/E balance…..collecting duct
Act of Micturition • Urine moves from the kidneys through ureters via peristaltic waves into bladder. • Bladder fills & detrusor muscles sense pressure • Structures and functions for voluntary control of voiding: -External sphincter- restrain or interrupt act -Conscious brain- starts act -Intact spinal cord- needed or else message from the brain is not received.
Hmmm…. • Why are UTIs more common in women than in men? Urethra in women = 1.5 to 2.5 inchesUrethra in men = 6 – 8 inches
Alterations in Urinary Function • Incontinence- brain is not receiving impulse or loss of external sphincter control • Retention- distended bladder due to nerve impulses not perceived or muscles unable to function
Amount1200 ml/day average Color OdorSee Next Slide pH 4.6 – 8.0 Turbidity Specific gravity1.010 – 1.025 Constituents Characteristics of Urine
Get a partner…AND • Describe to them what normal urine smells like. Ammonia? Concentrated urine d/t lack of adequate water intact ORPresence of bacteria in urine ORStanding urine (urea converts to ammonia when exposed to oxygen) Eau D’ Asparagus? Asparagus contains a sulfur compound called mercaptan. (It's also found in rotten eggs, onions, garlic, and in the secretions of skunks.) When your digestive tract breaks down this substance, by-products are released that cause the funny scent. Sweet? Uncontrolled Diabetes Musty? Liver Disease
Food/fluidintake + loss Developmental factorsSee Next Slide Stress Activity/Muscle tone Life style Medications ??? Factors That Affect Voiding
Geriatric Considerations • Decreased ability of kidneys to concentrate urine and decreased bladder capacity = nocturia • Decreased muscle tone of bladder = increased frequency • Decreased bladder contractility & stasis= increased frequency of UTI • Changes in cognition and mobility (in some)= increased incontinence issues
Assessing Urinary Status • Usual patterns • Recent changes • Difficulties • Artificial Orifices
Kidneys: R kidney located 12 rib L kidney lower Tenderness during palpation at costoverterbral angle? Bladder: Below symphysis pubis Supine position to examine Observe-roundness Palpate-tenderness, how high it distends Percussion- full bladder dull sound Physical Assessment
Assessment: Lab Results • Urinalysis- WBC, RBC, protein, glucose, bacteria = abnormal constituents • BUN (blood urea nitrogen) end product of protein metabolism… 10-20 mg/dLIncreased BUN (azotemia) signifies impaired kidney function… affected by diet (hi protein intake) and fluids (dehydration)Decreased BUN signifies impaired liver functionMany drugs elevate BUN (antibiotics, lasix +++)
Assessment: Lab Results • Serum creatinine - by product of muscle metabolism…excreted entirely by kidneys… Normal = 0.5-1.2 mg/dLIncreased levels signify renal impairment • BUN: Creatinine ratio- 20:1… when both rise together indicates kidney failure or disease
Anuria Dysuria Enuresis Frequency Glycosuria Hematuria Hesitancy Frequency Incontinence Nocturia Oliguria Polyuria Pyuria Retention Urgency Proteinuria Altered Urinary Functioning Terms to Know
NCLEX Question Your client has a urinary tract infection. Which of the following signs/symptoms would you expect the client to exhibit? • Proteinuria • Dysuria • Oliguria • Polyuria
Assessing Urinary Retention • Feeling of fullness • Voiding small amounts< 50 ml • Normal intake/inadequate output • Distended bladder • Discomfort • Bladder ScanIf > 300 ml should catheterize
Nursing Dx R/T Urinary Elimination • Impaired urinary elimination • Urinary retention • Functional urinary incontinence • Overflow urinary incontinence • Stress urinary incontinence • Reflex urinary incontinence • Urge urinary incontinence • Total urinary incontinence • Risk for infection r/t urinary retention and/or urinary catheterization • Risk for impaired skin integrity r/t urinary incontinence • Situational low self esteem r/t incontinence
Outcome Criteria Patient will: • Empty bladder completely at regular intervals • Decrease episodes of incontinence • Maintain regular urinary elimination pattern • Develop adequate Intake/Output • Have decreased dysuria
Nursing Interventions • Maintain voiding habits • Promote fluid intake • Strengthen muscle toneKegels 30-80/day • Stimulate urinationAuditoryTactile
Toilet Commode Bedpan Urinal Disposable“ Hat” Fx pan Safety Concerns Female Hygiene Interventions: Toileting
Interventions for Urinary Incontinence • Bladder training/ Habit training • External urinary device- Condom Catheter • Indwelling catheter-LAST resort
Condom Catheter (Texas Cath) • Rubber condom placed on penis of incontinent males • Connects to drainage bag to collect urine • Easy to apply and observe • Comfortable • Doesn’t require intubation • Prevents skin irritation from incontinence
Condom Catheter • Check every 2-4 hrs. • Remove and replace every 24 hrs. • Maintain free urinary drainage • Never tape to skin • Leave 1-2 inch space at tip of penis • Secure snuggly but not too tight • Follow manufacturer instructions
Urinary Catheterization Used to: • Keep bladder deflated during surgery • Measure residual urinePVR (post void residual) should be < 50 ml • Relieve retention • Obtain sterile urine specimen May use either: • Straight catheter or indwelling catheter
Indwelling catheter Refer to Lab Worksheet • Catheter inserted into urinary meatus through urethra into bladder to drain urine • Last resort as it introduces microbes into bladder…leading to UTI (urinary tract infection) • Performed using sterile technique...MD order needed • Remains in place via inflated balloon ALSOSuprapubic Catheter – diverts urethraUrologic Stents- temporary in ureters permanent in urethraIleal Conduit – diversion of ureters to ileum and stoma; requires appliance
Medications Affecting Urinary Elimination • Antibiotics …work against infectionBactrim, Levaquin, Cipro • Urinary antispasmotics …relieve spasms with UTIDitropan, Pro-Banthine • Diuretics….increase urinary outputLasix, Diuril • Cholinergics…increase muscle tone & functionUsed for urinary retention, neurogenic bladderUrecholine
Urinary Specimen CollectionRefer to Lab Worksheet • Routine urinalysis • Clean-catch/midstream urine • Sterile specimen ( catheterization or from indwelling catheter) • 24 hr. urine
Evaluating Urinary Elimination • Frequency • Amount • Ease/Difficulty • Color • Appearance • Odor
Complete Intake and Output Exercise • Handout