Download

1 / 25
280 likes | 390 Views
Chapter 3 Intrauterine Fetal Development The growth and development of the fetus is typically divided into three stages: Pre embryonic (ovum) stage (fertilization to 2-3 weeks):

E N D
Chapter 3 • Intrauterine Fetal Development • The growth and development of the fetus is typically divided into three stages: • Pre embryonic (ovum) stage (fertilization to 2-3 weeks): • The concepts is called an ovum during the period from conception until primary villi appear 12-14 days after fertilization or 4 weeks since LMP. • Rapid cell division and differentiation was occurred • Develop embryonic membrane. • The inner cell mass of blastocyst forming fetus that the cells differentiate into three primary gems layers: • The ectoderm (ecto = outside) • Gives skin, nails, tooth and nervous system. • The endoderm (endo =inner) • Gives the epithelial inner lining of GIT, respiratory system, endocrine glands and auditory canal. • The mesoderm (meso = middle) • Gives the connective tissue, muscle, blood and vascular system.
Embryonic Stage: 4-8weeks of gestation • Start from the end of ovum stage until 8 weeks of gestation (or 10 weeks since LMP) when the ovum measure approximately 3 cm. • The most critical stage of physical development as highly vulnerable to teratogenic agents as virus, radiation, infections or drugs. • Developmental interference during this stage leads to congenital anomalies. • Organogenesis taken place in this stage as the next:
The first system to function is the cardiovascular. • The blood vessels formation begins early in the third week. Heart start to pump blood at 4th weeks. • Fetal heart rate: 120-160 beat per minute. • Fetal circulation: the single umbilical vein carries oxygenated blood from the placenta. The paired umbilical arteries return most of the mixed blood from the fetus to the placenta. • The lungs begin to growth as a part from upper digestive tract at 4th weeks not functional until after birth. A substance called surfactant forms in the lungs at 27th week . • Alimentary tract is formed at 4th week but function not accomplished before delivery. • The kidneys develop rapidly at 5th week and begin to function and passing urine at 8th week.
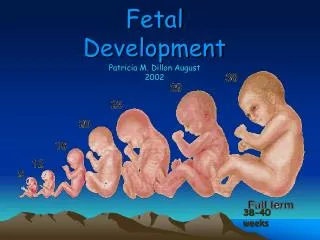
The fetus is covered with a white, creamy substance (skin) at the 18th week and at 20th week; the fetus is covered with lanugo hair. • CNS begins to develop at 3rd week. The neural tube complete closure at the 4th week. • External genitalia are well enough developed to be easily distinguished at the 12th week . • Fetal Stage: 9 weeks after conception until birth • Its start from the end of embryonic stage until delivery of fetus. • Fetus in Latin word = offspring. • There is a changes but not dramatic as in the preceding stages. • Every organ system and external structure is presented during this stage. • The fetus can be detected by trans-vaginal ultrasonography as early as 4 weeks after the last menstrual period and by trans abdominal ultrasonography in the second trimester.
Fetal heart sounds can be heard with a fetoscope by 18 to 20 weeks of gestation and by electronic Doppler can detect heart motion at 10 weeks of gestation. • The fetus is less vulnerable to teratogenic agents but may interrupt normal functional development of organs particularly the brain. • Assessment of Growth • Assessment of infant' growth is crucial during different stages of life because periodic assessment of infants and children permits early detection of growth deficiencies and deviations from normal standards. During assessment the midwife should take the following points in her consideration: • Physical growth assessment is usually carried out using tables and charts. • The measurements which are commonly done are weight, length , head circumference. Newly chest circumference is done for newborns to assess fetal growth at birth.
There is wide range of normal variation among infants and children of the same chronological age. These normal differences are described in terms or percentiles. Comparison of the child percentile with those of the previous examination of the same child can detect abnormalities in his growth. • Not all measurements of the same child necessarily fall into the same percentile, but each measurement should follow its own percentile in a healthy child. • Methods to Evaluate Growth • Charts: compare to norms • Compare to self over time • X rays • Teeth • Length , weight, head circumference • Size of head and legs: length of bones
Assessment of Development • Denver Development Screening Test II (DDST) • Screening test – not a measurement of intelligence • Used to identify children whose development deviation • It includes 4 areas of development • Personal social (such as smiling). • Fine motor adaptive (such as grasping and drawing). • Language (as ability to hear , to follow directions and to speak) and • Gross motor (such as walking). • Ages covered by the tests range from birth to six years. • Assessment of maturity • The process of maturation is continuous throughout life; it begins at conception and ends at death. • Maturational "events" include those aspects of maturation that occur once and provide an unambiguous signal that the individual has reached a particular level of maturity. For example, the exact age at which menarche (the first menstrual period) is experienced in girls or the exact the age of peak height velocity during the adolescent growth spurt. • The maturity process of a child can be assessed at a single examination using three aspects: • Sexual
The Denver Developmental Screening Test (DDST), commonly known as the Denver Scale, is a test for screening cognitive and behavioral problems in preschool children. • The scale reflects what percentage of a certain age group is able to perform a certain task. In a test to be administered by a pediatrician or other health or social service professional, a subject's performance against the regular age distribution is noted. Tasks are grouped into four categories (social contact, fine motor skill, language, and gross motor skill)
and include items such as smiles spontaneously (performed by 90% of three-month-olds), knocks two building blocks against each other (90% of 13-month-olds), speaks three words other than "mom" and "dad" (90% of 21-month-olds), or hops on one leg (90% of 5-year-olds). • The test was first introduced in 1967, and a revised as Denver II in 1992. It was widely used, and translated for use in twelve different languages. It has proven to be reliable, but its validity has been questioned and it has fallen out of favour with some organizations.
Sexual maturity can be assessed from the development of public hair in each sex, the genitalia in males and the breast in females. Usually, these assessments accomplished by with direct inspection. • Skeletal maturity is assessed from radiographs of wrist and is recorded as a continuum of skeletal ages (years) that may range from birth to 18 years. • Dental maturation is best assessed by taking panoramic radiographs of the mandible and maxilla and scoring the stages or formation and calcification of each tooth. • Catch-up growth • Unusual acceleration of growth may follow the recovery of infant or the child from a disease. • Catch-up growth (acceleration) is complete if the growth data for a child return to child's original percentile before the deficit occurred.
Catch-up growth is not always complete, however, and appears to depend on the timing, severity, and duration of the insult. This appears to be particular true in the treatment of hormone deficiencies. • Complete catch-up is more common in infants than in older children but in may be delayed. • Catch-up can occur in weight an any age, in stature until the time of epiphyseal fusion, and in head circumference until the sutures of the cranial vault interlock at about 5 years. • Growth velocity chart • is used to assess a child's growth rate over several periods of time. • Calculate your child's growth rate by recording his/her height at 2 points in time that are at least 150 days apart; then compare it with the normal growth rate of children the same age and sex.
Growth Chart • Growth charts are the primary tools for the recognition of unusual growth. Consist of a set of smoothed curves for selected percentiles with accompanying tables of means and standard deviations. • Some of these charts were developed from nationally representative samples to obtain estimates for total populations. The curves are usually for that 3rd, 5th. 10th. 25th, 50th, 75th, 90th, 95th, and 97th, percentiles. For example, when there are 100 children in an age group, the 3rd percentile value depends upon only the smallest three to four observations. • Children whose measurements fall within the 5th and 95th percentiles are generally considered within the normal growth range. Sudden or sustained changes in percentile may indicate a chronic disorder, emotional difficulty, or nutritional intake problem. These findings require further assessment or the physical status of the child as well as other types of evaluations such as dietary intake or serum laboratory measurements.