Download

1 / 26
350 likes | 1.54k Views
ATLANTOAXIAL INSTABILITY. Atlantoaxial Joint. Atlanto-Axial Joint. Atlantoaxial Instability (Subluxation). Signs Toy and miniature breeds Reluctance to be patted on head Neck pain May have tetraparesis (weakness in all 4 limbs) or tetraplegia (paralysis in all 4 legs)

E N D
Atlantoaxial Joint Atlanto-Axial Joint
Atlantoaxial Instability (Subluxation) • Signs • Toy and miniature breeds • Reluctance to be patted on head • Neck pain • May have tetraparesis (weakness in all 4 limbs) or tetraplegia (paralysis in all 4 legs) • Sudden death due to respiratory paralysis • Diagnosis— • Radiographs: lateral x-ray of neck in slight ventroflexion • avoid further spinal cord damage with positioning
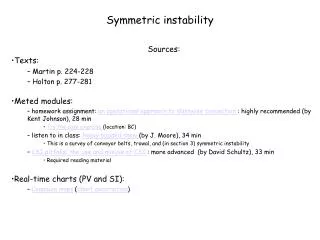
Atlantoaxial Instability (Subluxation) Normal toy breed dog Toy breed dog with atlantoaxialsubluxation CT scan: dens is marked by * Narrowed spinal canal X-rays of same dogs; note separation of C1 and C2 when dog’s neck is flexed in B
Atlantoaxial Instability (Subluxation) • Treatment— • Medical • splint neck in extension with cage confinement x 6 w • treat like other spinal cord trauma • Surgical (if unresponsive to medical Rx) • stabilize/decompress • attach dorsal process of axis to arch of atlas • fuse atlas and axis joint with pins and bone graft • hemilaminectomy to relieve spinal cord compression • Client info— • prognosis is fair to good for animals with mild signs • animals should not be used for breeding; may be hereditary
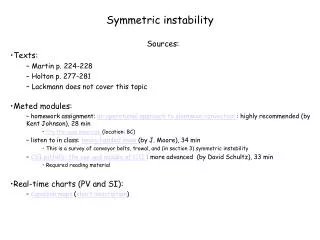
Atlantoaxial Instability: Surgical Correction Stabilization using trans-articular screws Stabilization using screws and bone cement
Cervical Spondylomyelopathy: Wobbler • Cervical spinal cord compression as a result of caudal vertebral malformation or misarticulation. • Large breed dogs (Great danes and Dobermans) • Signs • Progressive hind-limb ataxia (wobbly gait) • Pelvic limbs cross each other when walking • Abduct widely/tend to collapse • May drag toes (wears dorsal surface of nails) • Impaired proprioception • Signs may also be present in front limb • Crouching stance with downward flexed neck • Rigid flexion of neck; may have neck pain
Cervical Spondylomyelopathy: Wobbler • Dx • Radiographs to show malalignment and narrowing of spinal canal • Myelogram is essential to locate the region of compression • CT and MRI if available
Cervical Spondylomyelopathy: Wobbler • Rx—without treatment, prognosis is poor • Medical • Anti-inflammatory doses of corticosteroids • Neck brace • Cage confinement • Surgical • Decompression of spinal cord by laminectomy • Stabilize vertebral column • screws and wire dorsally • spinal fusion ventrally
Cervical Spondylomyelopathy: Wobbler • Client info • Prognosis is guarded • Most likely a hereditary disease • Multiple levels of compression less favorable prognosis than a single area of compression • Surgery is risky and costly
Degenerative Myelopathy • Etiology—unclear • May be autoimmune response to antigen in nerv sys • Degeneration of white matter in ascending and descending tracts • Signs • Mainly in G Shep and Shep mixes (>5 yr) • Progressive ataxia and paresis of hind limbs • Loss of proprioception is first sign • Dog “falls down” when trying to defecate • Muscle wasting of back muscles along caudal thoracic and lumbosacral areas • Symptoms progress until animal is unable to support weight on hind limbs
Degenerative Myelopathy • Dx— • Neurologic Exam • ↓ proprioception • ↑ patellar reflexes • Lack of pain • Normal sphincter tone; normal panniculus (pin prick) reflex • Radiographs usually normal • Rx—none; symptoms will progress to paralysis • Client info— • Degenerative myelopathy is a progressive, incurable disease • Although symptoms are similar at early stages, it is a different disease from hip dysplasia • When dog cannot support weight, quality of life should be evaluated
Deafness: Causes • damage to auditory pathway • chronic otitis • rupture of tympanic membrane • damage to middle ear (ossicles) • damage to auditory nerve • hereditary or congenital • bull terriers, Dobes, Rotts, Pointers, blue-eyed white cats, Dalmations, Aust Heelers, Aust shepherds, Eng setters, Catahoula • related to drug therapy • aminoglycosides(gentamicin, streptomycin, kanamycin • topical polymyxin B • Chloramphenicol • Chlorhexidine w/ centrimide • normal old age—usually due to atrophy of nerve ganglia or cochlear hair cells
Deafness • Dx • Inability to rouse sleeping animal with loud noise (e,g,. blast from air horn) is diagnostic • Rx: No treatment is available in most cases • Hearing aids are available for animals, but most will not tolerate something in ear canal • Client info • Hearing loss is permanent • If hereditary, do not breed • Animals can be taught to hand signals rather than words • Animals should not be off leash when outside • Hearing aids are available for dogs but are usually not tolerated; would only be appropriate for hearing impaired
Laryngeal Paralysis • 3 types (always be cautious of laryngeal paralysis because of the chance of rabies) • Hereditary: seen in Bouvier des Flandres and Siberian Huskies • Seen at 4-6 mo of age • Acquired: can occur from lead poisoning, rabies, trauma, inflammation of vagus nerve • 1.5 to 13 yr of age • Idiopathic: seen in middle-age to old large- and giant-breed dogs; castrated dogs and cats have a higher incidence than female and non-neutered males
Laryngeal Paralysis • Signs: • Inspiratorystridor • Resp distress • Loss of endurance • Voice change • Dyspnea/cyanosis/complete respcollapse • Dx: laryngoscopywill show laryngeal abductor m. dysfunction • Rx: surgical intervention including: • Arytenoidectomy • Removal of vocal folds • Client info: prognosis is guarded to good; do not breed if hereditary
Megaesophagus • Causes-lack of esophageal peristalsis (3 types): • Hereditary—a gene for the disease is identified in wire-haired fox terriers and min schnauzers • Congenital—Great Danes, German Shepherd, Irish Setters, Newfies, Sharpeis, Greyhounds (no gene ID’ed) • evident about weaning time when solid food is introduced • Due to incomplete nerve development in esophagus • Acquired—may be seen at any age; Pbtox; may be associated with neuropathies (e.g., myasthenia gravis, tick paralysis) • Signs • Regurgitation of undigested food • Respiratory problems (aspiration pneumonia) • Lack of growth
Megaesophagus Dx—barium swallow Esophagus is 3 times normal diameter
Megaesophagus • Rx • Elevated feeding (on platform, stairs) • Liquid or soft diet high in calories • Give several small feedings daily • Gastrostomy tube (long term) is an option • Client info • Prognosis—guarded to poor • Treatment aim is to reduce clinical signs and prevent aspiration pneumonia • There is no cure
Tick Paralysis • Cause—female tick (Dermacenter variablis, D. andersoni) → salivary neurotoxin • Neurotoxin interfered with Ach at neuromuscular jct • Not seen in cats; humans are affected • Signs— • Gradual onset of voice changes and hind-limb ataxia (motor deficit) progressing to a flaccid, ascending paralysis (1-3 d) • Sensation is intact • Ticks on the dog • Rx • Remove ticks (manually or with dip) • Usually resolves in 1-3 d • Supportive care until dog recovers • Ventilation required for resp paralysis
Coonhound Paralysis (Polyradiculoneuritis ) -thought to be an immune response to an unknown etiologic factor in raccoon saliva -some dogs will get it 1-2 wk after exposure, others exposed to same raccoon will not • Signs: similar to tick paralysis and rabies • Weakness begins in hind limbs with paralysis progressing rapidly to a flaccid tetraplegia • Alert, afebrile animal • Loss of spinal reflexes (patella tap, etc) • Loss of voice; labored breathing; inability to lift head • May die of respiratory failure • May last for 2-3 mo (usually good Px) • Rx: supportive nursing care • Client info • Dogs can be affected without exposure to raccoon • May require long-term nursing care • Some animals will regain total function, while more severely affected animals may not
Idiopathic Facial Nerve Paralysis • Etiology—unknown • Occurrence • Cocker Spaniels, Corgis, Boxers, Eng Setter, DLH cats • Signs— • Older dogs (>5 y) • Ear droop • Lip paralysis • Sialosis (drooling) • Deviation of nose • Collection of food in paralyzed side of mouth • Absence of menace and palpebral reflex
Idiopathic Facial Nerve Paralysis • Rx—efficacy of corticosteroids unknown • Artificial tears to prevent corneal ulcers • Keep oral cavity clear of food • Client info— • Cause is unknown • Complete recovery does not usually occur • May develop keratoconjunctivitis sicca (dry eye) • Animals may require life-long maintenance