Download
1 / 38
380 likes | 415 Views
This analysis from the Elderly Deceased Donor Kidney Allocation Working Group discusses the allocation of kidneys from elderly deceased donors in the UK. It covers donor age trends, discard rates, dual transplantation possibilities, and selection strategies for optimal organ utilization. The study aims to identify principles for potential incorporation into future kidney allocation schemes based on outcomes of transplants from elderly donors.

E N D
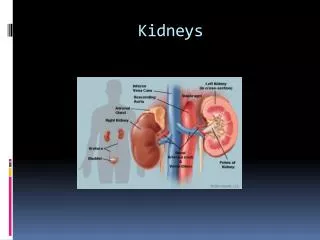
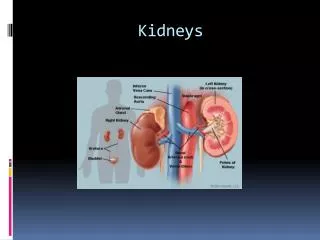
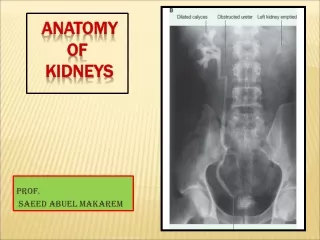
Allocation of elderly deceased donor kidneys A preliminary analysis from the Elderly Deceased Donor Kidney Allocation Working Group Lisa Bradbury, Niaz Ahmad, Paul Gibbs, Richard Baker, Adam McLean, Chris Callaghan Renal Transplant Services Meeting, 24 March 2015
Introduction • Rationale • Terms of reference • Analyses • Conclusions
Rationale Age of deceased donors in the UK, 2002-2012
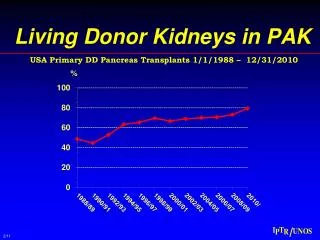
Median donor age by donor type, 1 Apr 2004 – 31 Mar 2014
Proportion of high risk (>1.35) kidney donors,1 Apr 2004 – 31 Mar 2014
Discard rate of retrieved kidneys, 1 Apr 2004 – 31 Mar 2014 Kidney fast-track scheme
Discard rate of retrieved kidneys from deceased donors, Apr 2009 – 31 Mar 2014
Discard rate of retrieved kidneys from DBD donors, Apr 2009 – 31 Mar 2014
Discard rate of retrieved kidneys from DCD donors, Apr 2009 – 31 Mar 2014
Rationale • Changing deceased donor demographics and patterns of organ usage • Need to minimise discard and optimise organ utilisation • No existing mechanisms to identify kidneys suitable for DKT • Changing age thresholds for regional DCD schemes?
Terms of reference • To review outcomes of transplants from elderly donors to determine whether allocation of a single kidney is always appropriate, and, if not, to identify which kidneys could be allocated for dual transplantation. • If current allocation is not deemed appropriate, to identify the appropriate recipient group for such kidneys. The aim would be to produce a set of principles, or a scheme, that might be easily incorporated into the next kidney allocation scheme.
Analysis – DKT in the UK • Heterogeneous indications, varying between centres (and surgeons) • Donor age, co-morbidities, eGFR, prolonged CIT • Gross appearance • Histological analysis • Perfusion parameters • No widely accepted recipient selection criteria • >60 years old, dialysis >1 year? • Cardiorespiratory and technical considerations
Number of kidney transplants, 1 Apr 2004 – 31 Mar 2014
Number of dual kidney transplants, Apr 2008 – Mar 2014
Age group for single and dual transplants, Apr 2008 – 31 Mar 2014
Graft survival by transplant type, 1 Apr 2004 – 31 Mar 2014 % Survival N SKT (donors≥60) 91% (90-92) 2610 DKT (donors≥18) 90% (85-93) 225 p=0.5 After risk-adjustment, no difference in 1-yr graft survival between SKT 60+ and DKT (p=0.32)
Patient survival by transplant type, 1 Apr 2004 – 31 Mar 2014 % Survival N SKT (donors≥60) 94% (93-95) 2327 DKT (donors≥18) 92% (87-95) 216 p=0.15
1 year eGFR by transplant type and donor age, 1 Apr 2008 – 31 Mar 2014 DBD DCD After risk-adjustment, 1-yr graft function (CKD stage) was better in DKT vs SKT 60+ (p=0.01)
Analysis – selection strategies • Donor age, co-morbidities, eGFR, prolonged CIT • Gross appearance • Histological analysis • Perfusion parameters
Analysis – selection strategies Donor age – 1-yr graft survival by donor type and donor age, 1.4.08-31.3.14 DCD DBD % survival N SKT (donors 60-64) 93 585 SKT (donors 65-69) 90 534 SKT (donors 70+) 86 367 DKT 93 53 % survival N SKT (donors 60-64) 93 444 SKT (donors 65-69) 90 410 SKT (donors 70+) 93 266 DKT 88 175
Analysis – selection strategies Donor age – 1-yr recipient eGFR by donor type and donor age, 1.4.08-31.3.14 DBD DCD
Analysis – selection strategies Donor age and co-morbidities – UKKDRI Watson CJE et al, Transplantation 2012
Analysis – selection strategies Median (IQR) UKKDRI of discarded kidneys, SKT (donors >60 yrs), and DKT, 1.4.04-31.3.14
Analysis – selection strategies UKKDRI – 1-yr graft survival by donor type and UKKDRI (donors >60 yrs), 1.4.08-31.3.14 DBD DCD Mean (SD) UKKDRI all DKT = 1.7 (0.4), all SKT = 1.2 (0.4) % survival N SKT (dri<1.5) 92 443 SKT (dri1.5-1.6) 90 320 SKT (dri1.6-2) 89 463 SKT (dri>2) 92 256 DKT 93 53 % survival N SKT (dri<1.5) 89 231 SKT (dri1.5-1.6) 94 318 SKT (dri1.6-2) 92 336 SKT (dri>2) 91 216 DKT 88 175
Analysis – selection strategies UKKDRI – 1-yr recipient eGFR by donor type and UKKDRI (donors >60 yrs), 1.4.08-31.3.14 DCD DBD Mean (SD) UKKDRI all DKT = 1.7 (0.4), all SKT = 1.2 (0.4)
Analysis – selection strategies New UKKDQI (nUKKDQI) 1.1.06-31.12.10, training dataset n=4034, validation dataset n=2689, 23% from donors aged >60 years nUKKDQI = exp{(0.01976*donor age) + (0.32727*history of cardiothoracic disease) - (0.00241*(donor eGFRadm x BSA/1.73))}
Analysis – selection strategies New UKKDQI (nUKKDQI)
Analysis – selection strategies New UKKDQI (nUKKDQI)
Kidney allocation criteria for DKT unable to be identified Is there a valid alternative approach?
Analysis – alternative strategy • Rather than offering for DKT, offer both kidneys and let the centre decide usage • SKT x 2 or DKT • DBD donor: offer to national centre with highest-ranking patient • DCD donor: offer to regional centre with highest-ranking patient • Which metric? • Impact on CIT?
Discard rate of retrieved kidneys from deceased donors, Apr 2009 – 31 Mar 2014
Conclusions • Kidneys from elderly deceased donors are increasingly common, but with a high rate of discard • DKT may be a valid strategy to increase utilisation • Using data available, no clear metric to identify kidneys best used as DKT • Limitations • Alternative strategy proposed • Recipient selection not yet addressed
Systems elsewhere • US • ECD program no longer (Dec 2014) – KDPI • OPTN dual kidney criteria (2 or more) • Age >60 • eGFR <65 ml/min on admission creatinine • Creat >220 μmol/L • Long-standing HT or DM • 15%<glomerulosclerosis<50% • Local/regional offering if KDPI >85% • Inconsistent offering practices (Tanriover B, AJT 2014)
Systems elsewhere • Eurotransplant Senior Program • Donors 65 years or older • Loco-regional, no HLA • 2013 – 515/2967 (17%) • Outcomes (Frei U, AJT 2008) • Shorter wait, less CIT, less DGF • More AR • Worse GS and PS c.f. O/A, A/O • Benefits for younger patients…
Current UK allocation policies • DBD NKAS • Always single kidney offered, regardless of donor age • Age points: = -1/2 (donor-recip age difference)2 • DCD regional allocation by donor age • Outside London: >50 years retained locally (x 5 years/year?) • London: >65 years offered as pair • Influence of KFTS • Maximum flexibility • If one kidney accepted by non-KFTS centre?