Download
1 / 27
270 likes | 440 Views
Cardioprotective Effects of Postconditioning in Patients Treated with Primary PCI Evaluated with Magnetic Resonance. Jacob T Lønborg

E N D
Cardioprotective Effects of Postconditioning in Patients Treated with Primary PCI Evaluated with Magnetic Resonance Jacob T Lønborg Niels Vejlstrup, Erik Jørgensen, Steffen Helqvist, Kari Saunamäki, Peter Clemmensen, Lene Holmvang, Marek Treiman, Jan S Jensen, Henning Kelbæk, Thomas Engstrøm Department of Cardiology Rigshospitalet Copenhagen Denmark
Presenter Disclosure The authors have no disclosures with regard to the conduct of this study
Background Zhao et al., 2003
Background Zhao et al., 2003
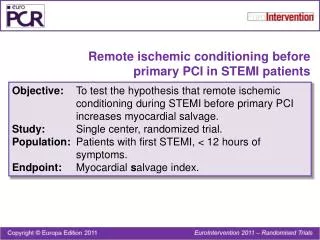
Background Postconditioning has been suggested to reduce myocardial damage during PPCI in patients with ST-segment elevation myocardial infarction (STEMI) However clinical experience is limited
Occluded Reperfusion coronary artery Conventional treatment Post- conditioning 30 30 30 30 30 30 30 30 sec Balloon inflations - deflations Postconditioning
Postconditioning STEMI - PPCI Randomization Conventional treatment Postconditioning Balloon inflation 30 sec / reperfusion 30 sec Balloon inflation 30 sec / reperfusion 30 sec Balloon inflation 30 sec / reperfusion 30 sec Balloon inflation 30 sec / reperfusion 30 sec Continue standard treatment Continue standard treatment
Major inclusion criteria • Patients who presented with symptoms and • signs of their first STEMI • Chest pain for less than 12 hours • TIMI 0-I (range 0-III) in the infarct related artery
Major exclusion criteria • History of a previous myocardial infarction • Left main stenosis • Spontaneous reperfusion before intervention (TIMI II-III) • Multivessel disease (any other stenosis > 70%) • Cardiogenic shock • Stent thrombosis
Endpoints • Primary: • Infarct size measured with CMR 3 months after the initial • procedure (analysis blinded)
Endpoints • Secondary: • Cardiac death after 1 and15 months • Clinical status after 3 months (angina, heart failure) • TLR during hospitalization, after 1 and 15 months • Re-infarction during hospitalization, after 1 and 15 months • LVEF by CMR
Flow Chart Screened patients 530 Eligible patients 118 Did not meet inclusion criteria 412 2 deaths • 123 TIMI > 1 before PCI • 64 no myocardial infarction • 44 multiple vessel disease • 39 linguistic problems • 28 duration of symptoms >12 hours • 28 cardiogenic shock • 27 did not meet inclusion criteria • 23 unconsciousness • 17 refused to participate • 12 stentthrombosis • 11 vessel unsuitable for postconditioning • - 24 no reason reported 30 lost to CMR - 15 logistic problems - 6 claustrophobia - 3 pacemaker implantation - 3 nephropathy - 3 technical difficulties 86 patients for CMR 116 patients for 3-month clinical follow-up
Baseline clinical demography Post- conditioning n = 59 Conventional Treatment n = 59 p Mean age (yrs) Male gender (%) Diabetes (%) Hypertension (%) Treatment for hyperlipidemia (%) Current smoker (%) Family history of CAD (%) Previous myocardial infarction (%) Previous PCI (%) Symptom onset to balloon (min) Time to CMR (days) Use of GP IIb/IIIa inhibitor (%) Use of bivalirudin (%) 61 69 7 37 46 61 37 10 7 241 ± 149 83 ± 20 83 7 62 74 7 32 41 49 31 7 8 255 ±196 84 ± 18 83 12 ns ns ns ns ns ns ns ns ns ns ns ns ns
Baseline clinical demography Post- conditioning n = 59 Conventional Treatment n = 59 p Mean age (yrs) Male gender (%) Diabetes (%) Hypertension (%) Treatment for hyperlipidemia (%) Current smoker (%) Family history of CAD (%) Previous myocardial infarction (%) Previous PCI (%) Symptom onset to balloon (min) Time to CMR (days) Use of GP IIb/IIIa inhibitor (%) Use of bivalirudin (%) 61 69 7 37 46 61 37 10 7 241 ± 149 83 ± 20 83 7 62 74 7 32 41 49 31 7 8 255 ±196 84 ± 18 83 12 ns ns ns ns ns ns ns ns ns ns ns ns ns
Baseline angiographic results Post- conditioning n = 59 Conventional Treatment n = 59 p Number of Diseased vessels (%) 1 Vessel Disease 2 Vessel Disease 3 Vessel Disease Infarct related artery (%) LAD RCA LCX / PDA / PLA/ OM / D TIMI 0-I before procedure Visible thrombus (%) 78 15 7 44 47 8 100 75 83 14 3 39 42 19 100 83 ns ns ns ns
Baseline angiographic results Post- conditioning n = 59 Conventional Treatment n = 59 p Number of Diseased vessels (%) 1 Vessel Disease 2 Vessel Disease 3 Vessel Disease Infarct related artery (%) LAD RCA LCX / PDA / PLA/ OM / D TIMI 0-I before procedure Visible thrombus (%) 78 15 7 44 47 8 100 75 83 14 3 39 42 19 100 83 ns ns ns ns
Procedural Results Post- conditioning n = 59 Conventional Treatment n = 59 p Type of stent (%) None BMS DES Number of stents (%) 0 1 2 3 Diameter of final balloon, mm Length of stented segment, mm Max deployment pressure, mmHg Thrombectomy (%) TIMI grade III after procedure (%) 15 6 78 15 71 12 2 3.3 19.6 17.6 10 95 17 12 69 17 68 14 2 3.3 18.1 16.2 14 88 ns ns ns ns ns ns ns
Procedural Results Post- conditioning n = 59 Conventional Treatment n = 59 p Type of stent (%) None BMS DES Number of stents (%) 0 1 2 3 Diameter of final balloon, mm Length of stented segment, mm Max deployment pressure, mmHg Thrombectomy (%) TIMI grade III after procedure (%) 15 6 78 15 71 12 2 3.3 19.6 17.6 10 95 17 12 69 17 68 14 2 3.3 18.1 16.2 14 88 ns ns ns ns ns ns ns
CMR – late enhancement = Infarct mass = LV mass Infarct (%) = Infarct mass / LV mass
CMR – The wavefront phenomenon Myocardium at risk Final infarct 3 hours 96 hours 40 minutes
= Infarct = None-infarct AAR-ESA = Infarct / (none-infarct + Infarct) CMR – Area At Risk Basis 1 2 3 4 5 6 7 8 Apex Ortiz-Pérez et al., 2007
Results - CMR p=0.007 p=0.987 p=0.007 p=0.037
Results - CMR Lønborg et al., 2010
Results - CMR Infarct size - interaction test p=0.705 AAR = Area At Risk
Clinical outcome at 3 months Heart failure Angina pectoris p=0.048 p=0.362 7
Clinical outcome at 3 months Post- conditioning n = 59 Conventional Treatment n = 59 p Myocardial infarction, n (%) STEMI NSTEMI Stent thrombosis, n (%) Pacemaker, n (%) PCI on target vessel, n (%) CABG, n (%) Death, n (%) 0 (0) 3 (5) 0 (0) 1 (2) 0 (0) 0 (0) 2 (3) 0 (0) 1 (2) 1 (2) 2 (3) 1 (2) 1 (2) 0 (0) ns ns ns ns ns ns ns
Conclusion • Postconditioning reduces infarct size in patients with STEMI • Postconditioning improves functional class in patients with STEMI • The treatment is independently effective for all Areas At Risk • Postconditioning should be tested in larger clinical trials