Download
1 / 43
430 likes | 661 Views
Out-of-Pocket Costs Associated with Childhood Immunizations. Noelle-Angelique Molinari, PhD Health Economist National Immunization Program, CDC. Collaborators. Rich Schieber, MD, MPH Mark Messonnier, PhD. Background. NIS Data: Georgia.

E N D
Out-of-Pocket Costs Associated with Childhood Immunizations Noelle-Angelique Molinari, PhD Health Economist National Immunization Program, CDC
Collaborators • Rich Schieber, MD, MPH • Mark Messonnier, PhD
Strongly recommends reducing out-of-pocket (OOP) costs to increase vaccination rates Suggests this may be accomplished by: Providing free vaccine Reducing administration costs Providing insurance coverage Reducing copayments at POS Guide to Community Preventive Services
Benefits of Lower OOP Costs • Increased coverage • Law of Demand • price decline leads to increased quantity demanded • 13 studies* show decrease OOP associated with increase coverage • Encourages medical home for all care • IZ more prompt & timely * Briss PA et al. Reviews of evidence regarding interventions to improve vaccination coverage in children, adolescents, and adults. Am J Prev Med 2000;18(1S):97-140
Problems of Higher OOP Costs • Multiple IZ providers, esp. health depts. • Lower coverage rates • Push to seek care outside medical home • Disparity in OOP costs may directly result in disparity in coverage
Purpose • To estimate OOP costs associated with childhood IZ: • Under current standards of care received at medical home • For a defined, large, heterogeneous population • To determine whether disparities exist by • Insurance status • Payer types
Assumptions: Optimal Care • Georgia 2003 birth cohort • No change in insurance distribution across age or over time • Full compliance with AAP 2003 vaccine schedule • Each child receives current standard of care in medical home • Each child receives shots as soon as eligible
Assumptions: Optimal Care • 7 visits from birth through age 4 • Each private MD visit includes well-child exam, vaccine, and administration fee • No new combination vaccines used • No submitted charges are disallowed by insurance • No shortages • Relative prices remain constant over time
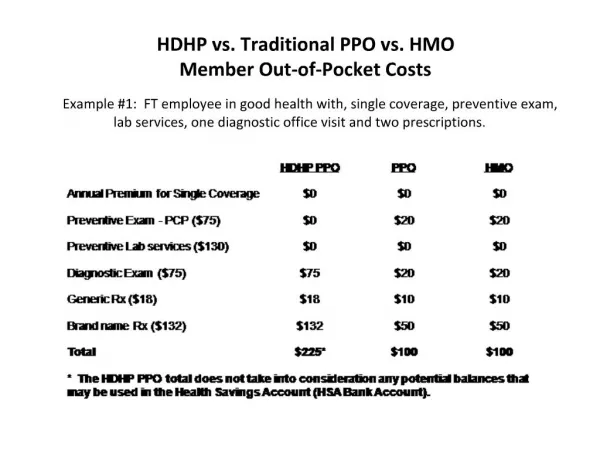
Total Cost per Visit Total Cost = (WC Exam Fee) + (Vax Fee) + (# Vax) (Vax Admin Fee) • WC Exam = Well-child exam fee • Vax Fee = Vaccine price to patient • # Vax = No. of vaccines given that visit • Vax Admin Fee = Fee charged for administering shot
Out-of-Pocket (OOP) Cost per Visit OOP = Copay(WC Exam)+ Copay(Vax) + Copay(Vax Admin)(#Vax) • Copayment is the amt. of total charges a patient pays • Copay can be either: • Flat fee ($10) • Rate (10%)
Example: Private Insurance6 mo old HepB, DTaP, Hib, IPV, PCV
Per-Child Cost • Sum all costs over 7 visits • Discount to obtain present value of per-child cost in 2003 dollars
Cost for Georgia 2003 Cohort • Multiply • OOP cost-per-child for each insurance category • # children in that insurance category (CPS 2004 data) • Result is population-weighted estimate of OOP costs associated with childhood immunization for Georgia’s 2003 birth cohort
Costs Associated with Immunization 2003 Georgia Birth CohortUninsured Go to Private MD
Costs Associated with Immunization 2003 Georgia Birth CohortUninsured Go to Health Dept
OOP Costs & IZ Coverage • Coverage negatively correlated with OOP costs * Phil Smith provided information from NIS 2003 on GA IZ coverage rates by plan type.
Data are Not Perfect • HIP Enrollment survey 61% response (enrollment per plan) • Tricare weights are estimated, not based on enrollment • Copayments are based on benefit plan descriptions rather than actual reimbursements (except Large group)
Implications… • Decreasing OOP costs will increase coverage • Plan designs are skewed toward low OOP costs • VFC reduces OOP cost & thereby reduces insurance-based disparities • Uninsured still face high OOP costs • Medicaid & SCHIP low OOP cost encourages IZ among low income children
Policy Implications • Are child vaccinations (not just vaccines)based on an entitlement or a discount program? • How might IZ coverage change with decreased availability of public health clinics? • Funding is not keeping pace with Medicaid/ SCHIP expansion. How will this affect IZ coverage?
Payments & Copays by Visit • Individual & Small Group
Payments & Copays by Visit • Large Group
Payments & Copays by Visit • Tricare
Payments & Copays by Visit • Medicaid & Peachcare
Payments & Copays by Visit • Medicare & Uninsured
Cost per Child • Calculated present value of 7 visits using 3% discount rate with monthly basis • r = 3%, m = 12 • Burden in today’s dollars of childhood vaccinations from birth through age 4
Total & OOP Costs per visit by Insurance type in Georgia, 2003
Discounted Total & OOP Costs per Child by Insurance type in Georgia, 2003