Download

1 / 24
240 likes | 586 Views
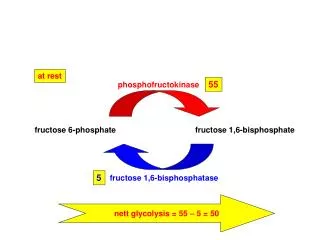
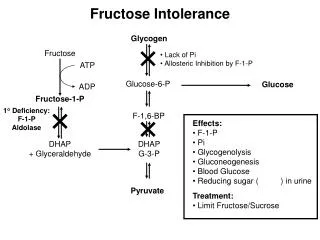
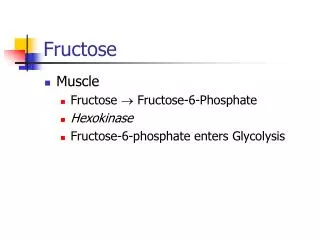
Fructose Metabolism. ATP ADP. ATP ADP . 2) dihydrous aceton PO 4. + Glyceraldehyde-3-PO 4. Phospatase. F-1-PO 4. F-1,6 diPO 4. Isomerase . Phospatase. G-6-PO 4. Glucose . Fructose . 1) Glyceraldehyde. F-1-PO 4.

E N D
ATP ADP ATP ADP 2) dihydrous aceton PO4 +Glyceraldehyde-3-PO4 Phospatase F-1-PO4 F-1,6 diPO4 Isomerase Phospatase G-6-PO4 Glucose Fructose 1) Glyceraldehyde F-1-PO4 It is converted into glucose in liver and intestine .
CHO | H-C-OH | R CH2OH | H-C-OH | R CH2OH | C=O | R NADHph + H+ dehydrogenase Aldose reductase Glucose Sorbitol Fructose NADNADH+H - Essential Fructosuria :Inherited due to deficiency of Fructokinase enzyme ( benign ) .- Hereditary Fructose Intolerance :Deficiency of aldolase B accumulation of Fructose-1-Phosphate which decrease phosphorylase enzyme of glycogenolysis which lead to hypoglycemia .
UDP - Galactose ( Activedonnes) :1- Glycolipid synth.2- Lactose formation .3- Mucopolysaccharide.4- glycosaminoglycone ( GAGs ) . Conversion of Glucose into Galactose :
Blood Glucose • Plasma Glucose level: • Fasting level 70-110 mg/dl. • one hour after meal 120-150. • two hours after carbohydrate meal (post prandial ) till 140. Galactosemia it is the increase in blood glactose conc. due to inability to metabolize galactose.Causes: inherited enzymes deficiency A) Galactokinase. B) Galactose-1-p-uridyl transferase. C) Epimerase.Effects: 1- Cataract. 2- Liver failure. 3- Mental retardation.
Source of blood glucose: Factors that add glucose to blood1. Carbohydrate diet.2. Glycogenolysis.3. Gluconeogensis. 1. From C,H,O in diet. 2. Glucogenic compound.3. Propionate.4. Lactate ( in skeletal muscle and RBC ).5. Amino acid transferred from muscle to liver.6. Dietary carbohydrate e.g. starch.7. From liver glycogen through glycogenolysis (for 18 h fasting).8. Amino acid and other metabolites ( gluconeogenesis ). Liver and kidney can convert these substrates into glucose.
Regulation of Blood Glucoseblood glucose is maintained 70-110mg because:hyperglycemia (increase blood glucose) can cause cerebral dysfunction but its effect on extra cellular osmolarity.II. hypoglycemia cause impairment of cerebral function as brain is very dependent on blood glucose for energy Fructose remove glucose from blood1.uptake by tissue2. Excretion in urine 3. utilization a. oxidation b. lipogenesis c. glucogenesisetabolism
Regulation of Blood GlucoseRegulation of glucose1- hormonal 2- hepatic 3-renal 1)Hormonal regulation:
*Insulin:Insulin is hormone secreted by β-cell of langerhans of pancreas. It is only hormone which reduce blood glucose level.1. Transfer glucose into cells.2. Increase glycogen storage.3. Stimulate glucose oxidation.4. Decrease glycogen breakdown. 5. Decrease glyconeogensis.6. Increase lipogensis.
*glucagon:Hormone secreted by α cell of pancreas increase blood glucose by: 1. Increase glycogen breakdown by increase adenyl cyclase and increase glyconeogensis.2. Catechol amines : from suprarenal medulla ↑ blood glucose by : a) ↑ glycogenolysis b) ↑ glucose up take by liver 3. Glucosteroid as cortisol : by suprarenal cortex . ↑ blood G by : a) ↑ gluconeogenesis b) ↓ of glucose up take by tissues4. Growth Hormone secreted from anterior pituitary gland a) ↓ of G up take by tissue b) Blocks insulin action in all membranes.
2) Hepatic regulation 3) Renal regulation Blood glucose is filtered in glomular filtrate and reabsorbed again. * If blood glucose exceeds certain limit (180 mg/dl), glucose will increase and exceed the capacity of tubular enzyme to reabsorb. So it will appear in urine (called glycouria). Renal Threshold *In Fasting state:1.It add glucose to blood by glycogenolysis and gluconeogenesis. 2. Convert fatty acid ( acetyl CoA) → Keton bodies.*In Fed State : 1. Convert glucose into glycogen. 2. Convert Glucose into fatty acid
II) Hypoglycemia If blood glucose decreased (less than 45 mg/dl), that would cause cerebral dysfunction if prolonged cause death (so "GLUCAGON" must be taken) Symptoms : Headache, Confusion, Hunger, Anxiety, Slurred speech, palpitation Causes : 1. Fasting 2. due to organ disease : - Pancreatic: insulinoma (Tumor) - liver disease: hepatic carcinoma 3. Glycogen storage disease 4. Starvation 5. Adrenocortical disease (↓ epi) 1. Hyperglycemia:It is rise of blood glucose Causes:1. Diabetes Mellitus 2. Receive I.V. fluids containing glucose 3. Severe stress 4. In cerebro-vascular accidents5. Disturbance in hyperglycemic hormones
Stimulative:1. Drugs: overdose of insulin2. Overdose of oral hypoglycemic agents3. Liver poison as chloroform, alcohol4. Postgastrectomy (increase absorption of glucose)5. Galactosemia6. Hereditary lactose intolerance
It is a state of chronic hyperglycemia (Glucose urea). Relative or absolute deficiency of insulin hormoneBiochemical disturbance of diabetes mellitus1) Carbohydrate:↓Glucose uptake by tissue ↓oxidation ↑gluconeogenesis and↑glycogenolysis ↓intracellular glucose →hunger (polyphagia)* Increase blood glucose by: a) Increase plasma osmolarity → dehydration. b) Dehydration of brain cells (coma). c) Dehydration of body cells "thirst" (polydepsia). d) Glucose urea: frequent urination loss of vitamin B1 loss of K+, Na+ • Protein metabolism: • * Increase protein breakdown. • * Increase gluconeogensis (amino acid convert to glucose) • 1.phosphatase release • 2. excess breakdown of tissue protein (muscle wasting) • 3. decrease antibody. • 4. poor wound healing. Diabetes mellitus
3) Lipid metabolism:Excess lipolysis mobilization of free fatty acid and glycerol to tissue and liver lead to:1. lose weight. 2. hyperlipidemia (Athrosclerosis)3. fatty liver4. excess keton bodies (Ketonemia, Ketosis), which leed to ketotic coma, hyperkalemia4) Microangiopathy:Degeneration affected blood vessels of kidney and retina of eye. (renal failure, blindness.
1. glucose tolerance test 2. fasting blood glucose not more than 110 mg/dl 3. two hrs post (prandial) must be within the normal fasting level. 4. Glycosylated hemoglobin (HbA1C) it is a glycated protein which results from simple non enzymatic reaction between globin part of HB and glucose, its level in the red cells is directly proportional to the blood glucose level at the time of formation of such cell, this level remains as it for the whole life span of red blood cells 120 days * It is useful for monitoring the degree of control of diabetes mellitus during last 8-12 weeks before the test. Normal 4 - 7.2% 5. plasma fructose amine Albumin under go glycosylation 6. Microalbuminurea early detection of D.M. in urine by special kits. Diagnosis of Diabetes Mellitus
500 diabetic Glucose in blood 200 Renal threshold 180 100 normal 1 2 3 4 hours Glucose tolerance curve