Download
1 / 60
620 likes | 813 Views
Health and Demographic Surveillance System. Under-5 mortality known to be around 500/1000 in 1978. 1978-2010: Bandim Health Project (BHP): The need to do research during emergencies: A personal experience from Guinea Bissau. Mapping and numbering. Child list.

E N D
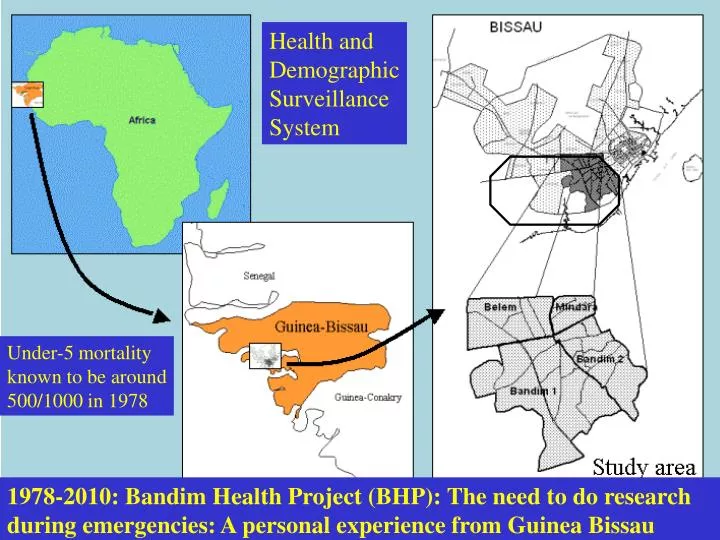
Health and Demographic Surveillance System Under-5 mortality known to be around 500/1000 in 1978 1978-2010: Bandim Health Project (BHP): The need to do research during emergencies: A personal experience from Guinea Bissau
Bandim Health Project 1978-2010:Strategy for routine data collection
Bandim Health Project Rural study areas 90,000: 3,500 newborns/year ANTULA BONO AEROPORTO VOLTA DE BISSAU ANTULA HAFIA COCO PLAQUE II PLUBA LUANDA PLAQUE I ST. LUZIA ROSSIO GRANJA / BRA CALEQUIR VETERINARIO National hospital Simao Mendes CUPILON PEFINE DE BAIXO AMEDALAI CUPILON BAIRRO DE TCHADA MILITAR CIMA SINTRA MEDINA NEMA REINO PENHA MISSIRA GAMBEAFADA CENTRO AJUDA II MINDARA VARELA BELEM CANAL DO GEBA QUELELE CHAO ILHEU DE DO REI CUNTUM PAPEL BANDIM 2 CUNTUM BANDIM 1 Urban study area 102,000: 3,000 newborns Personnel 150 WIM DEKKERS PSB, 1996
Children whose death might be prevented by measles vaccine are ...on the “road to death”, and their nutritional status is so poor that they are more likely to die of any infectious disease. Thus preventing a death with vaccine among these children may not necessarily save a life, but only change the cause of death (Mosley 1982) Sweden funded project to reduce malnutrition => mortality
Overcrowding and intensive exposure
War in Guinea-Bissau 1998-1999 • June 1998: President attempt to arrest the chief of the army – rebellion among officers. Takes the barrack controlling entry to the city • President invited troops from neighbouring Senegal and Conakry • Foreign troops and rebels used heavy artillery – in the city • Within two weeks – nearly every body had fled (except soldier, thieves, and very old people – and dogs and pigs) • Most people fled through Prabis – from 7,000 to 50-80,000 people • In the two largest villages the average number of people was 104 per house
WAR June 1998-May 1999 Pop increased from 7000 to 50-80,000
War and humanitarian aid- phase I • Services provided by BHP during the war (we had personnel, cars, some money – and displomatic car) • Buying diesel for pumping/distributing water • Buying drugs in Bissau • Organising clinics in major villages (doctors/students) – drugs to hospital • People in Dakar – sending money, drugs, satellite phone to Bijagos • Considered measles vaccination campaign but not done because coverage high and rainy season (few measles cases) • WFP storage in Bissau taken => Red Cross (in 3 weeks only reached 40%) • => BHP took over distribution – we reached everybody in 2-3 weeks • National Humanitarian Committee – conflict with Donors • BHP followed the internally displaced when they went back to the city
Food distribution took most of the resouces
Nutritional status and mortality of refugees and resident children • Method: 30 clusters of 14 children aged 9-24 months=420 children • 25% residents – and 41% from Bissau-BHP area (had pre-war data) and 34% Bissau-non-BHP • Measured reception of food aid, mid-upper-arm circumference (MUAC), rice consumption, and additional expenditure, mortality • 5 visits over 12 weeks (every 3 weeks) – initially in refugee area – subsequently also back in Bissau • Results: • MUAC: proportion low MUAC (<130mm) increased strongest i resident children; Growth: worse for resident children than BHP children; MUAC normalised for both refuges and residents when refugees left • Food consumptions: residents better – and staple for resident but declined for children returning to Bissau • Distribution: initially only refugees – then all • Mortality: Ratio Resident/Refugee = 4.5 (1.1-30) – over 12 weeks • Mortality: Ratio Refugee area/back at home= 7.2 (1.3-134) • Why more malnutrition and mortality among resident than refugees?
4th war War begins 2nd war 3rd war Ceasefire
War and humanitarian aid – phase II • After the first ceasefire the BHP followed the Bissau people back to the city – and organised: • In study area • Food distribution – conflict with Donors • Soap for hygiene • Treatment of malnourished children • Vitamin A distribution • Bed nets and impregnation • TB drugs Whole city of Bissau • Clinical consultations in all the health centres • Support for the hospital • Measles vaccination • Bednets to mothers of children <2 • Outbreak control (measles and meningitis) Post-war: • House reconstruction
Studies – and designs: • Search for determinants of mortality in emergency • Nutritional status – MUAC <130 mm most effective (cluster surveys during war – plus pre-war data) • Breastfeeding/weaning (Before-after) • Vaccination status (Before-after) • TB-infection – no treatment (Before-after) • HIV-infection (Before-after) • Effects of interventions in emergency • Treatment/prevention • Treatment of children at health centres (not evaluated) • Hospital treatment (Before-after) • Bednets (not evaluated) • Treatment of malnourished (monitoring during treatment) • Immune enhancement • Vitamin A (stepwise introduction) • Vaccinations campaigns (measles, meningitis) (not evaluated)
Irregular treatment of TB during war Mortality ratio (MR) in treatment war/peace cohort = 3.1 (1.2-8.1) Mortality ratio (MR) in treatment war/peace cohort (HIV+) =8.2 (1.6-41) (MR completed treatment: war/peace cohort = 1.3 (0.3-5.2))
Mortality for HIV-2 vs uninfected before and during the war, 1998-99
Breastfeeding and mortality during a 3-month war situation (children aged 9-20 mo)
Reduction in hospital case fatality: 42% (11-63) Children of mothers without schooling: 73%(27-90); with schooling: 33%(14-61)
Step-wedged design: gradual introduction Vitamin A versus no vitamin A yet: MR= 0.49 (0.1-2.7)
Measles vaccination Campaigns Dec 1998 Meningitis vaccination Campaign April 1999
Risk factors: Mortality during 3-month war in Bissau 1998 according to pre-war vaccination status (1-18 mo old) F/M mortality ratio: DTP 3.1 (1.1-8.6)
Natural experiment: Children randomised to measles vaccine orcontrol vaccine (IPV) just before war MV at 6 mo; MV at 9 mo Control= IPV at 6 mo; MV at 9 mo Measles vaccine IPV MRR= 0.30 (0.1-0.9) MRR= 0.28 (0.1-0.9) – without measles
War and humanitarian aid:Thinking with the stomach • The focus was on food distribution - not the most important • Nutritional status was not associated with family consumption • Mortality was not associated with family consumption • Mortality went down at the same time as nutritional intake went down • In a not malnourished population: general food distribution affects travelling patterns and thereby exposure to infections
Church distributed double rations
War and humanitarian aid:Thinking with the stomach • The focus was on food distribution - not the most important • Nutritional status was not associated with family consumption • Mortality was not associated with family consumption • Mortality went down at the same time as nutritional intake went down • In a not malnourished population: general food distribution affects travelling patterns and thereby exposure to infections • What we could have done better – disease prevention/treatment: • Bednet impregnation earlier (fight in the national committee) • Treatment malnourished children started earlier • TB drugs immediately (HIV drugs) • What we could have done better – immune enhancement: • Immunizations - BCG could have been given earlier; measles vaccine given earlier? • Encourage breastfeeding restart? • Vitamin A?
Post-war studies I: Why low mortality at the paediatric ward? • We first believed that it was mostly due to free drugs at the ward due to humanitarian aid => we and then WHO provided malaria treatment kits to all hospitalised children => did not lower mortality • Conducted trial of treatment monitoring. • All staff trained in standard protocol • One ward was closely monitored and personnel got a small supplement (50$/month) • Intervention group 5% (21/457) mortality vs control group (usual treatment) 10% (46/477) => relative risk: 0.48 (0.3-0.8)
Post-war II: RCT of MV at 4+9 mo (new) vs DTP3 at 4mo+MV at 9mo (current policy) Mortality rate 0.36(0.1-0.9) Exclude measles infect. 0.55 (0.4-0.9) 0.57(0.3-0.9) 0.51(0.3-0.8) Reduction in overall mortality: Two MV at 4 and 9 mo: 49% (22% to 68%)
Under-5 mortality in Bissau Under-5 mortality in Bissau Measles Vaccine (MV) EPI/PEV introduced BCG War MV campaign BCG at birth Early MV DTP4 HBV DTP
War and humanitarian aid:Thinking with the stomach • The focus was on food distribution - not the most important • In a not malnourished population: general food distribution affects travelling patterns and thereby exposure to infections • What we could have done better – disease prevention/treatment: • Bednet impregnation earlier (fight in the national committee) • Treatment malnourished children started earlier • TB drugs immediately (HIV drugs) Probably uncomplicated • What we could have done better – immune enhancement: • Immunizations - BCG could have been given earlier; measles vaccine given earlier? • Give measles vaccine at younger age • Encourage breastfeeding restart? • Vitamin A? Potentially more effective but also potentially negative
LBW-BCG RCT:Accumulated mortality curves for DTP vaccinated at 2 months of age and not DTP vaccinated children
Ghana VAST, reanalysis Original trial conducted in 1989-91; MRR=0.81 (0.68-0.98) (Lancet 1993) Not analysed by vaccination status Boys Girls VAS/placebo Mortality Ratio P<0.01 The VAS effect differed in girls with and without vaccinations Benn et al, Am J Clin Nutr 2009
Before-after measles vaccination: Mortality rate for children aged 6-35 months Measles vaccine Measles vaccine Before vs after: not selection bias. Only measles vaccine was introduced
Before-after measles vaccination: Annual mortality in African community studies More than 25 studies => Not prevention of acute or long-term measles mortality! => MV has beneficial non-specific effects
HT DTP/polio 1 2 3 measles 6 10 14 wk Birth 9 mo From 1985: African high-titre (HT) measles vaccination trials – in search of measles eradication • WHO had moved the age of measles vaccination to 9 months of age in early 1980s • High-titre Edmonston-Zagreb (EZ) measles vaccine could be given early at 4-5 mo of age BCG OPV
High-titre measles vaccine, Bissau, 1986-90, and Senegal, 1987-92 Guinea-Bissau Senegal EZ=HTMV at 4/5 mo; IPV at 9 mo Control= IPV at 4/5 mo; MV at 9 mo HTMV was fully protective
High-titre measles vaccine: 2-fold higher female mortality • Lessons from high-titre measles vaccine (HTMV) trials: • EZ HTMV was fully protective against measles infection • => negative non-specific effect • Vaccines can have sex-differential effects • Public health effects: excess mortality from 4 to 60 months • => if HTMV had no been withdrawn => at least ½ mill additional (female) deaths annually in Africa • WHO introduced HTMV 1989 and withdrew it in 1992 => • => Major donors: Money for new vaccines! => We looked for important NSEs and sex-differential effects of other vaccines => standard MV, BCG and DTP
Male and female mortality before and after measles vaccine in Senegal Bandafassi 1981-1988 Niakhar 1985-1988 F/M 1.04 (0.9-1.3) 0.65 (0.4-1.0) 1.02 (0.9-1.3) 0.63 (0.4-1.1) • Pre-vaccination no difference in F and M mortality. • MV particularly good for girls – • found in all subsequent studies
Mortality by vaccination status for children aged 0-6 mo at initial visit – 6 mo follow-up, rural areas BCG BCG+DTP No vaccine BCG+ / BCG- 0.55 (0.36-0.85) DTP+ / DTP- 1.84 (1.10-3.10) BCG # DTP BMJ 2000
DTP/OPV 1 2 3 BCG measles DTP+OPV boost OPV Birth 6 10 14 wk 9 mo 18 mo RCT: Testing NSE of BCG • BCG not given to LBW children => RCT justified • We recruited LBW children at maternity ward – 11/2004-1/2008 • Randomising to BCG-at-birth or later (current practice)
RCT of BCG-at-birth to LBW children: 2004-2008 Mortality rate MRR=0.83(0.6-1.1) MRR=0.55(0.4-0.9) 45% reduction in neonatal mortality – F: 49% M: 41% Not prevention of TB in first month => Beneficial NSEs of BCG Reduction in neonatal sepsis and respiratory infections
Hospital case fatality (%) F/M case fatality ratio inversion: BCG vs DTP; DTP vs MV
Female/male MR for DTP-vaccinated children DTP negative NSEs particularly for girls
DTP after HTMV? No DTP after HTMV DTP/IPV after HTMV F/M ratio: 1.93(1.3-2.8) F/M ratio: 0.96 (0.7-1.3) Withdrawn for the wrong reason? Change in sequence: DTP as last vaccination!
What can be done to reduce the negative effect of DTP? 1 1 2 2 Increased female mortality in the age groups of DTP => Change the immunological profile => RCT1: BCG revaccination (19mo) RCT2: Early MV (4½ m)
RCT1: BCG-revaccination vs nothing at 19 mo by vaccination statusMortality from 19 mo to 5 years of age Mortality rate MRR=1.78(1.0-3.0) MRR=0.36(0.1-1.0) P=0.006 I. BCG after booster DTP => expected beneficial effect II. Not taken into account: No DTP booster=> received DTP later BMJ 2010