Download
1 / 35
390 likes | 2.43k Views
High Frequency Ventilation in PPHN. Namasivayam Ambalavanan M.D. Division of Neonatology, Department of Pediatrics, University of Alabama at Birmingham. Overview of presentation. Introduction to PPHN Types of HFV Hyperventilation in PPHN HFOV, HFJV, and HFFI trials HFV techniques.

E N D
High Frequency Ventilation in PPHN Namasivayam Ambalavanan M.D. Division of Neonatology, Department of Pediatrics, University of Alabama at Birmingham
Overview of presentation • Introduction to PPHN • Types of HFV • Hyperventilation in PPHN • HFOV, HFJV, and HFFI trials • HFV techniques
What is the problem? • PPHN / PFC : persistence of the pattern of fetal circulation postnatally due to a sustained elevation of pulmonary vascular resistance, with right-to-left shunt at the ductus arteriosus or foramen ovale in the absence of structural heart disease • Incidence:1: 522-1454. Exact incidence unknown in the absence of ICD coding or a “gold standard” for diagnosis • Mortality and morbidity: mortality > 50% in the absence of ECMO, and >10-20% with ECMO; >20% severe handicap/intracranial hemorrhage/deafness (Walsh-Sukys. Clin Perinatol 20: 127-143, 1993)
Causes of PPHN PPHN (Geggel RL, Reid LM: Clin Perinatol 11:525, 1984) Normal Arterial Number Decreased Arteries e.g. CDH Normal muscularization Increased muscularization Maladaptation due to acute injury (commonest) e.g. Sepsis, MAS, asphyxia Developmental immaturity Chronic injury with vascular remodeling Malform- ation
Current management Confirm diagnosis of PPHN Correct underlying abnormalities (hypothermia, acidosis, hypocalcemia, hypoglycemia, polycythemia) Conservative mechanical ventilation Trial of hyperventilation If low PO2, trial of rescue therapies MetabolicHFV Surfactant Vasodilators ECMO Alkalosis NO, PGD2, PGI2, Tolazoline, Adenosine
Pathophysiological basis of current management • Mechanical ventilation: • V/Q matching to improve oxygenation • respiratory alkalosis to reduce PVR • Metabolic alkalosis: effect of pH on PVR • Vasodilators: specific relaxation of the pulmonary vasculature. Most experience with NO. • ECMO: modified long-term cardio-pulmonary bypass
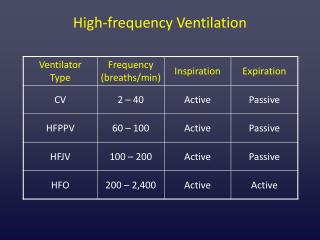
High frequency ventilation • Techniques HFPPV HFJV HFFI HFOV VT>dead sp > or < ds > or <ds<ds Exp passive passive passive active Wave- variable triangular triangular sine wave form Entrai- none possible none none ment Freq. 60-150 60-600 300-900 300-3000 (60-80) (350-450) (480-720) (600-900) (/min)
High frequency ventilation • HFPPV • conventional ventilators with low-compliance tubing • ventilatory rates of 60-150/min • not very effective: minute ventilation decreases with high frequencies [If TI < 3 TC, VT decreases.] (Boros et al. Pediatrics 74: 487-492, 1984 ) • ventilator and circuit design are not optimal for use at frequencies
High frequency ventilation • HFJV (e.g. Bunnell Life Pulse HFJV) • adequate gas exchange with lower MAP • Servo pressure reflects volume ventilated: • increases with improving compliance or resistanceor by peri-ET leaks • decreased by worsening compliance, resistance, obstruction, or pneumothorax • Larger babies: 300 bpm; smaller ones: 500 bpm
High frequency ventilation • HFJV (contd.) • MAP controls PaO2, DP (and frequency) controls PaCO2 (MAP controls lung volume. PaO2 will not respond to increased MAP if FRC normal) • smaller VT (DP) with higher PEEP better than larger VT with lower PEEP (--> hypoxia with hypocarbia) • Optimal PEEP: no drop in SpO2 when CMV off • Parallel conventional ventilation recruits alveoli (use low rate : 1-3 bpm; 0-1 bpm if air leak)
High frequency ventilation • HFOV (e.g. Sensormedics 3100A) • MAP controls PaO2, amplitude (and frequency) control PaCO2 • Optimal MAP difficult to determine as CXR “rib space counting” not accurate (Thome et al. Pediatr Pulmonol 26:265-72, 1998) • Frequency: 5-10 Hz better for CO2 elimination; 10-15 Hz better for improving oxygenation • maybe useful in airleak syndromes • maybe useful in PPHN; may decrease need for ECMO esp. if combined with NO
High frequency ventilation • HFFI (e.g. Infant Star with HFFI module) • active expiration in Infant Star model makes operation more like HFOV • MAP controls PaO2, amplitude (and frequency) controls PaCO2 • insufficient evidence to show it to be superior to conventional ventilation • more convenient: single ventilator for CMV and HFV makes initiation and weaning easier
High Frequency Ventilation in PPHN • V/Q matching to improve oxygenation • Respiratory alkalosis to reduce PVR • Improved response to inhaled NO • “Rescue” for air leak syndromes
Hyperventilation in PPHN No HV/Alk HV Alk HV+Alk p Mortality% 4.4 6.8 9.5 9.8 0.67 ECMO% 33.3 13.6 44.6 34.2 0.008 Duration 7.8 7.2 7.8 12.6 0.0013 ventilator (d) Duration O2 (d)11.1 11.5 11.9 17.5 0.001 O2 at 28 d 2.7 2.8 6.8 16.7 0.1 (Walsh-Sukys et al. Pediatrics 105:14-20, 2000)
HFOV in term infants • Early studies: Kohelet et al. Crit Care Med 16: 510-6, 1988 • HFOV in 41 infants with PPHN • 34 showed improved oxygenation and ventilation, and decreasing MAP Carter et al. Pediatrics 85: 159-64, 1990 • 50 ECMO referrals with A-a O2>600. 4 died early. • 21 responded to HFOV and did not require ECMO • 25 needed ECMO, with more morbidity & 3 died. • Infants responding to HFOV more often had pneumonia
HFOV in term infants Varnholt et al. Eur J Pediatr 151: 769-74, 1992 • HFOV tried in 50 infants meeting ECMO criteria • 25 responded to HFOV, 25 needed ECMO • 2 responders subsequently needed ECMO due to air leaks Responders in Carter’s and Varnholt’s study tended to be younger (37-38 wks vs. 39-40 wks)
HFOV in term infants • Recent studies: Clark et al. J Pediatr 124: 447-54, 1994 • GA >34 w, B.wt> 2 kg, < 14 d age on high vent settings • 81 neonates randomized to HFOV or CV • Patients stratified before admission based on primary diagnosis (pneumonia, MAS, RDS, air leak, or other)
HFOV in term infants Clark et al contd. • Mortality: HFOV 1/39 vs. CV 2/40 • ECMO need: HFOV: 12/39 vs. CV 6/40 (n.s) • Median days on ventilator: 8 in both groups • O2 reqt at 28 days: HFOV 11/39 vs. CV 5/40 (n.s.) This trial was prematurely terminated (needed 250) and hence did not have enough power
HFJV in term infants Carlo et al. Am J Dis Child 143: 233-8, 1989 • 14 infants on HFJV compared to 23 infants on CV • HFJV: reduction in MAP and PaCO2 • No change in mortality, A-aDO2, air leaks, BPD, duration of ventilation or O2 supplementation • This was a small pilot study, not a randomized trial Peters et al. J Perinatol 12: 21-4, 1992 • 2 infants with pulmonary hypoplasia and PPHN worsening on CV survived on HFJV
HFJV in term infants Engle et al. J Perinatol 17:3-9, 1997 • Small RCT of HFJV (n=11) vs. HFPPV • HFJV: Stable MAP and PIP. Improved oxygenation, ventilation, and OI • HFPPV: Required higher PIP to maintain same oxygenation, ventilation, and OI. • No difference in survival without ECMO, duration of ventilation, O2, hospital stay, need for ECMO, or BPD.
HFJV Stewart et al. Eur Respir J 9:1257-60, 1996 • 30 infants meeting criteria for ECMO • 22 responded to HFJV, 8 non-responders required ECMO • Responders showed a decrease in OI without increases in MAP within 4 hours • Same problem of small sample size, uncontrolled observational report Many similar uncontrolled studies and case series exist on HFJV, but only a few controlled trials in term infants.
HFFI in term infants • Very few trials of HFFI in term infants Jirapaet et al. Respir Care 46: 586-94, 2001 • 36 infants with PPHN requiring hyperventilation and FiO2 1.0 with PaO2 < 60 torr. HFFI (n=18) or CV (n=18) in non-randomized manner. • HFFI: • Survival 78% vs. 44% on CV (p=0.087) • Less chronic lung disease (1 vs. 5, p 0.02) • Faster extubation (8.1 vs. 18.7 d, p 0.03) • Improvements in other respiratory variables (less hypocarbia and alkalosis, improved oxygenation)
Comparison of HFV techniques • No human comparisons Wiswell et al. Am J Dis Child 146: 1287-93, 1992 • 56 newborn piglets with meconium instillation • Randomized to CV, HFJV, or HFFI for 6 hours • Measures of oxygenation mostly similar • Lung histologic changes worse on CV compared to HFJV or HFFI Simma et al. Pediatr Pulmonol 22: 263, 1996 • More lung injury in animals treated with HFV+CV than HFOV alone
Comparison of HFV techniques Bancalari et al. J Pediatr 110-617-22, 1987 • Animals on HFOV vs. HFJV • More air trapping on HFJV (due to active exhalation on HFOV?) Many centers now use HFOV for term infants with PPHN, rather than HFFI or HFJV Not possible to state if one type of HFV is better in human infants
HFV Indications • Usually used as “rescue” therapy for infants not improving/deteriorating on conventional ventilator • Response to HFJV or HFOV may depend on disease pathophysiology: • Pneumonia and RDS more likely to respond (70-90%) • MAS (50%) and CDH (20%) less likely to respond (Baumgart et al. Pediatrics 89:491, 1992; Paranka et al. Pediatrics 95: 400, 1995; Stewart et al. Eur Respir J 9:1257, 1996)
HFV techniques • HFOV, usually with Sensormedics 3100 • MAP: 1-3 cm H2O higher than on IMV • Frequency: 10-12 Hz • Inspiratory time: 33% • Amplitude: sufficient for visible chest motion • Target ABG: pH 7.45-7.55, PaCO2 30-40, PaO2 80-100, HCO3 26-30
HFV techniques • “High volume strategy” often used • Useful in animal models and preterm infants with RDS • Assessment of lung volume a problem (chest X-Rays not accurate) • Initial MAP 10-20% more than MAP on IMV. • Increase MAP in 1-3 cm H2O increments until oxygenation and a/A ratio improve or cardiac compromise occurs • FiO2 can then be weaned. As lungs improve, wean MAP slowly (MAP changes may take > 1 hr to affect PaO2)
HFV + NO • The combination of HFOV and NO is more effective than HFOV alone or NO alone Kinsella et al. J Pediatr 131: 55-62, 1997 • Mulicenter RCT on PPHN with n=205 • Randomized to IMV+NO or HFOV alone • If PaO2<60, cross-over to other therapy • If PaO2 still <60, HFOV+NO • Treatment success if PaO2>60 sustained
HFV + NO Kinsella et al contd. • 28% responded to NO, 23% to HFOV (100% survival and similar outcome in responders) • Non-responders following crossover: 21% responded to NO, and 14% to HFOV • 125 did not respond to either NO or HFOV alone: 32% responded to HFOV+NO • Combination works better for those with significant parenchymal lung disease (e.g. MAS, RDS)
HFV + Surfactant • Surfactant: • inactivation in MAS and pneumonia • deficiency in RDS and CDH • Animal studies • HFV does not affect delivery of bolus surfactant (Heldt et al. Pediatr Res 31:270, 1992; Walther et al. Pediatr Res 22:725, 1987) • HFV and surfactant prevent lung injury synergistically (Jackson et al. Am J Respir Crit Care Med 150: 534, 1994)
HFV + Surfactant • Survanta in term infants study group: • Multicenter RCT on infants at risk for ECMO • Surfactant use may reduce need for ECMO, especially when used early (OI 15-22) (Lotze et al. J Pediatr 132:40-7, 1998) • Surfactant in MAS: • 1/20 in surfactant gp vs. 6/20 controls needed ECMO • 0/20 in surfactant gp vs. 5/20 controls had air leaks (Findlay et al. Pediatrics 97: 48-52, 1996)
HFV + Surfactant • No studies focusing on HFV + Surfactant in term neonates • Studies in preterm neonates indicate that HFV: • prolongs efficacy of surfactant • reduces number of surfactant doses • reduces pulmonary morbidity (Gerstmann et al. Pediatrics 98:1044, 1996; Clark and Gerstman. Clin Perinatol 25: 113-122, 1998)
Does HFV “rescue” prevent ECMO but lead to more chronic lung disease? Vaucher et al. J Pediatr 128: 109, 1996 • ECMO survivors vs. avoiders: less CLD, shorter ventilation and hospital stay Walsh-Sukys et al. J Pediatr 125: 104, 1994 • ECMO survivors vs. avoiders: less CLD, less rehospitalizations however, Schwendeman et al. Crit Care Med 20: 372, 1992 • ECMO avoiders had less CLD and neurologic morbidity
Impact of HFV: more recent reports • Reduction in ECMO use by HFV + NO • Magnitude of reduction ranges from 40 to 75%, depending on center • Reduction of ECMO use not associated with longer ECMO in those needing it • Shorter hospitalization, lower costs (Kennaugh et al. J Perinatol 17: 366-9, 1997; Kachel et al. Int J Artif Organs 18: 589-97, 1995; Hintz et al. Pediatrics 106: 1339-43, 2000)
The current situation: Despite common use of HFV, there is insufficient data from randomized controlled trials to support the routine use of rescue HFV in term infants with PPHN