Download
1 / 1
10 likes | 152 Views
fMRI in BODY INTEGRITY IDENTITY DISORDER. Sheryl Foster 1,2 Mayuresh Korgaonkar 3 Lavier Gomes 1,2 Michael Graf 4 Anthony Harris 1,2 Chris Ryan 1,2 1 Westmead Hospital 2 The University of Sydney, 3 Brain Dynamics Centre & Westmead Millenium Institute, 4 GE Healthcare: Australia.

E N D
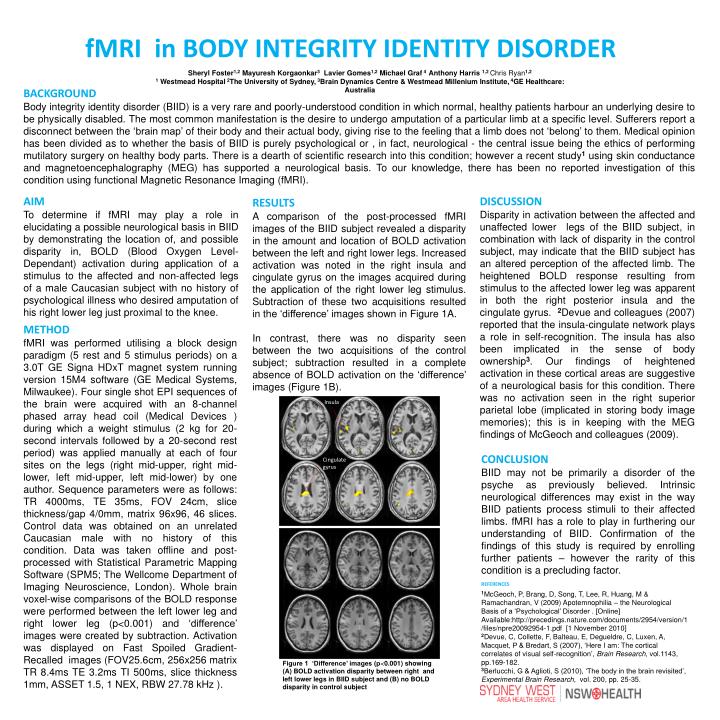
fMRI in BODY INTEGRITY IDENTITY DISORDER Sheryl Foster1,2Mayuresh Korgaonkar3Lavier Gomes1,2 Michael Graf 4 Anthony Harris 1,2 Chris Ryan1,2 1Westmead Hospital 2The University of Sydney, 3Brain Dynamics Centre & WestmeadMillenium Institute, 4GE Healthcare: Australia BACKGROUND Body integrity identity disorder (BIID) is a very rare and poorly-understood condition in which normal, healthy patients harbouran underlying desire to be physically disabled. The most common manifestation is the desire to undergo amputation of a particular limb at a specific level. Sufferers report a disconnect between the ‘brain map’ of their body and their actual body, giving rise to the feeling that a limb does not ‘belong’ to them. Medical opinion has been divided as to whether the basis of BIID is purely psychological or , in fact, neurological - the central issue being the ethics of performing mutilatorysurgery on healthy body parts. There is a dearth of scientific research into this condition; however a recent study1using skin conductance and magnetoencephalography (MEG) has supported a neurological basis. To our knowledge, there has been no reported investigation of this condition using functional Magnetic Resonance Imaging (fMRI). AIM To determine if fMRI may play a role in elucidating a possible neurological basis in BIID by demonstrating the location of, and possible disparity in, BOLD (Blood Oxygen Level-Dependant) activation during application of a stimulus to the affected and non-affected legs of a male Caucasian subject with no history of psychological illness who desired amputation of his right lower leg just proximal to the knee. DISCUSSION Disparity in activation between the affected and unaffected lower legs of the BIID subject, in combination with lack of disparity in the control subject, may indicate that the BIID subject has an altered perception of the affected limb. The heightened BOLD response resulting from stimulus to the affected lower leg was apparent in both the right posterior insula and the cingulate gyrus. 2Devue and colleagues (2007) reported that the insula-cingulate network plays a role in self-recognition. The insula has also been implicated in the sense of body ownership3. Our findings of heightened activation in these cortical areas are suggestive of a neurological basis for this condition. There was no activation seen in the right superior parietal lobe (implicated in storing body image memories); this is in keeping with the MEG findings of McGeoch and colleagues (2009). RESULTS A comparison of the post-processed fMRI images of the BIID subject revealed a disparity in the amount and location of BOLD activation between the left and right lower legs. Increased activation was noted in the right insula and cingulate gyrus on the images acquired during the application of the right lower leg stimulus. Subtraction of these two acquisitions resulted in the ‘difference’ images shown in Figure 1A. In contrast, there was no disparity seen between the two acquisitions of the control subject; subtraction resulted in a complete absence of BOLD activation on the ‘difference’ images (Figure 1B). METHOD fMRI was performed utilising a block design paradigm (5 rest and 5 stimulus periods) on a 3.0T GE Signa HDxT magnet system running version 15M4 software (GE Medical Systems, Milwaukee). Four single shot EPI sequences of the brain were acquired with an 8-channel phased array head coil (Medical Devices ) during which a weight stimulus (2 kg for 20-second intervals followed by a 20-second rest period) was applied manually at each of four sites on the legs (right mid-upper, right mid-lower, left mid-upper, left mid-lower) by one author. Sequence parameters were as follows: TR 4000ms, TE 35ms, FOV 24cm, slice thickness/gap 4/0mm, matrix 96x96, 46 slices. Control data was obtained on an unrelated Caucasian male with no history of this condition. Data was taken offline and post-processed with Statistical Parametric Mapping Software (SPM5; The Wellcome Department of Imaging Neuroscience, London). Whole brain voxel-wise comparisons of the BOLD response were performed between the left lower leg and right lower leg (p<0.001) and ‘difference’ images were created by subtraction. Activation was displayed on Fast Spoiled Gradient-Recalled images (FOV25.6cm, 256x256 matrix TR 8.4ms TE 3.2ms TI 500ms, slice thickness 1mm, ASSET 1.5, 1 NEX, RBW 27.78 kHz ). A Insula CONCLUSION BIID may not be primarily a disorder of the psyche as previously believed. Intrinsic neurological differences may exist in the way BIID patients process stimuli to their affected limbs. fMRI has a role to play in furthering our understanding of BIID. Confirmation of the findings of this study is required by enrolling further patients – however the rarity of this condition is a precluding factor. Cingulate gyrus B REFERENCES 1McGeoch, P, Brang, D, Song, T, Lee, R, Huang, M & Ramachandran, V (2009) Apotemnophilia – the Neurological Basis of a ‘Psychological’ Disorder . [Online] Available:http://precedings.nature.com/documents/2954/version/1/files/npre20092954-1.pdf [1 November 2010] 2Devue, C, Collette, F, Balteau, E, Degueldre, C, Luxen, A, Macquet, P & Bredart, S (2007), ‘Here I am: The cortical correlates of visual self-recognition’, Brain Research, vol.1143, pp.169-182. 3Berlucchi, G & Aglioti, S (2010), ‘The body in the brain revisited’, Experimental Brain Research, vol. 200, pp. 25-35. Figure 1 ‘Difference’ images (p<0.001) showing (A) BOLD activation disparity between right and left lower legs in BIID subject and (B) no BOLD disparity in control subject






















