Download
1 / 24
240 likes | 460 Views
Interim PACS Data Sharing – RCR PACS and Teleradiology special interest group Jerry Norman, PACS Technical Lead 21 November 2006. Context. Clinical Need The growing imperative PACS deployment model Where we are going Current PACS/RIS release schedule. Clinical Need.

E N D
Interim PACS Data Sharing – RCR PACS and Teleradiology special interest groupJerry Norman, PACS Technical Lead21 November 2006
Context • Clinical Need • The growing imperative • PACS deployment model • Where we are going • Current PACS/RIS release schedule
Clinical Need .. (Extract from a growing number of letters) • ‘We are writing regarding the problems we have been experiencing in setting up an electronic link between the {Trust A} and {Trust B’s} PACS systems. Although {Trust A} and {Trust B} are separate trusts, in many ways they work as one very large hospital (e.g. with Radiotherapy, Paediatrics and Maternity at {Trust B} and Vascular Surgery, Urology and Interventional Cardiology at {Trust A}, all providing services for both hospitals). This entails a lot of patient movement between the two trusts. • It is essential for safe patient care to have all of these patients’ imaging available at both trusts. It is also essential to be able to compare {Trust A} and {Trust B} imaging at both sites using a single interface. {Trust A} and {Trust B} share a common PMS and a dedicated 100Mbps link already exists between the 2 trusts. Preliminary talks with the 2 PACS vendors have revealed that it would be technically possible to connect the 2 PACS systems so that both trusts’ images were seamlessly accessible at both sites. • Connecting for Health (CFH), apparently on the grounds of security, is currently blocking this plan’.
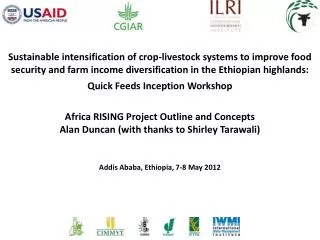
2006 2007 2008 2005 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 R1 COTS Central Data Store NE & EEM R2 (Initial Security SSO/ RBAC/Spine) LRS/PC Rel (Final Security) R3 Clinical(PSIS Integration) Dates tba R1 COTS COTS (Gemini) SOC & NWWM R2 Security Release (SSO/RBAC/LRS/PC/Spine + CRS integration) R3 - Clinical (PSIS Integration) Dates tba Key : PACS only -Accenture / Agfa (Impax & Agility) PACS/RIS - FJA/CSCA / GE Centricity & HSS CRIS PACS/RIS release schedules
Image sharing policy • Policy purpose • Short term policy • Healthcare communities • Short term mechanisms • Short term controls
Policy purpose The policy document: • is an interim measure, outlining NHS CFH’s short term PACS image sharing policy • defines mechanisms Trusts may use for data sharing, until the deployment of the PACS/RIS Spine security release • does not outline technical solutions - shows what can be done not how it can be done • will no longer stand, once the PACS/RIS Spine Security release is in place between sharing systems
Key Concept • The implementing of image sharing mechanisms is limited to the local boundaries within which a Healthcare Community (HC) operates • local systems, processes and policies which will effectively control and audit patient consent and legitimate access to shared data • Image sharing must be limited to within a Healthcare Community
NHS Organisation 1 Defined Healthcare Community between NHS Organisation 1 within PACS Entity A and NHS Organisation 2 within PACS Entity B for Image Sharing required to support a defined business Process Q. PACS Entity A Mutually agreed and documented image sharing protocol in line with this Policy. NHS Organisation 2 PACS Entity B Healthcare community 1
Defined Healthcare Community between NHS Organisation 1 within PACS Entity A and NHS Organisation 2 within PACS Entity B for image sharing required to support the defined business process Q NHS Organisation 1 PACS Entity A Mutually agreed and documented Image Sharing Protocol for business process Q Mutually agreed and documented Image Sharing Protocol for business process Z NHS Organisation 2 PACS Entity B Defined Healthcare Community between NHS Organisation 1 within PACS Entity A and NHS Organisation 2 within PACS Entity B for Image Sharing required to support the defined business Process Z Healthcare community 2
Defined Healthcare Community between NHS Organisation 1 within PACS Entity A, NHS Organisation 2 within PACS Entity B and NHS Organisation 3 within PACS Entity C for Image Sharing required to support a defined business process Q PACS Entity A NHS Organisation 1 NHS Organisation 2 NHS Organisation 3 PACS Entity B PACS Entity C Mutually agreed and documented Image Sharing Protocol Healthcare community 3
Short term mechanisms • where available and supported, the following image sharing mechanisms can be facilitated: • point-to-point sender initiated ‘push’ DICOM image transfer, for example via Teleradiology products • secure removable media • web accessing another PACS entity’s local data store within a healthcare community • DICOM query/retrieve from another PACS Entity’s local data store
Short term controls • Before data sharing can take place: • an ACF addressing IG requirements in controlling access to patient identifiable data must be in place (using a combination of technical, business process and policy controls) • there must be an audit of the end-to-end process • error correction must be extended to include all users who may have accessed an image as a result of data sharing • the transit of patient identifiable data must be secure
Trust/LSP engagement • Controls should be implemented using technology wherever possible • LSP systems will be involved in most if not all Image sharing activity, and will need to be configured to maximise the available technology to support the interim controls • A number of pilot activities are being progressed within the programme and LSP engagement will be required with these pilots • Trusts/Entities/SHA’s are already approaching LSPs for interim solutions (this will increase) and requesting • Secure DICOM connectivity to devices outside of the entity domain • Development of Web access etc • Provision of compatible removable media solutions
Healthcare Community NHS Organisations sharing PID are responsible for ensuring adherence to relevant Information Governance, DoH Policy, relevant legislative requirements and the NHS Care Record Guarantee In order to achieve this Image sharing Protocols must be established between the organisations between which PID is being exchanged. A Data Sharing Protocol provides a mechanism by which sharing organisations can formally document sharing activity and associated control mechanisms which have been mutually agreed between them. NHS Organisation 1 PACS Entity A NHS Organisation 2 PACS Entity B
National Level Cluster Level • Legislation • DoH Policy • CFH policy • Solution specific guidance • CFH IG Guidance • Solution Specific Protocol Templates • Solution Specific Policy and Procedure HC Data Sharing Protocol • Defines bounds of the Healthcare Community • Clinical requirement sharing • Details the technical, business process and policy control mechanisms in place
Next steps • Image sharing protocol template – available mid-December • provides a template format and appropriate completion guidance to Trusts implementing data sharing activities as part of a health care community • Common policy and procedures document – available end Dec • Information governance in line with ISO27001 • A number of image sharing pilots are underway
Current activity • Pilots overview • Pilots matrix • Southampton • Aintree
Progress so far.. Aintree ISTC integration. • CFH have engaged with Aintree to gather requirements: • Key issue: • Mobile modality, provided by an ISTC to acquire images and later, ISTC reports. • Images and reports required back at Trust • Solution required in time for LSP's PACS/RIS Golive - 5/2/2007. • LSP RIS to ISTC RIS integration is required in order for the Trust to obtain the full benefit of the service and reduce clerical error. • Options being considered for image transfer are CD, DICOM push or LSP PACS to ISTC PACS. • The ISTC Radiologists may require to see previous imaging held within LSP PACS in order to maintain the quality of reports CFH are aware of a similar pilot being undertaken by Kent and Medway, Information Governance issues require resolving by the Trust, LSP, DH and CFH
Progress so far.. Southampton • CFH Engaged with Southampton to gather requirements: • Key Points: • Large Tertiary site - Images required from around 15 sites across the Southern Cluster to support Opinions, Referrals and MDTMs • Most images are not required on the Local PACS. SUHT want to avoid unspecified images on the local PACS to limit Administrative overhead. • Solutions provided by FJA - favoured solution (RA600) selected and being developed. • Host RA600 configured at Southampton. • Referring organisation will push images to host RA600 from DICOM end point. • Q/R from Southampton host RA600 to some organisations may be required. • Separate web server being investigated to work in conjunction with Host RA600 to serve images within Southampton via second Icon on desktop to those who require it.
Challenges • Contractual position • NHS number • Leveraging the Cluster Data Stores • Keeping the report and image together • Variations in RIS provision • Integrating ISTCs • Existing System Providers