Download
1 / 12
130 likes | 314 Views
Amphetamine Toxicity. AM Report 8/10/09 Mike Contarino. Learning Points. 1. Hyperthermia has a broad differential, and drugs of abuse should be kept in mind. 2. Watch for rhabdomyolysis, DIC, and multiorgan failure after hyperpyrexia.

E N D
Amphetamine Toxicity AM Report 8/10/09 Mike Contarino
Learning Points • 1. Hyperthermia has a broad differential, and drugs of abuse should be kept in mind. • 2. Watch for rhabdomyolysis, DIC, and multiorgan failure after hyperpyrexia. • 3. Amphetamines result in dopamine, NE, and serotonin release, catecholamine surge!
Hyperthermia Differential • Sepsis • Encephalitis • Meningitis/Brain Abscess • NMS • Malignant hyperthermia • Pheochromocytoma • Thyroid storm • Tetanus • EtOH/Benzo withdrawal • Salicylate/Li toxicity • Sympathomimetic toxicity • Serotonin syndrome • Anticholinergic Toxicity • Hypothalamic Stroke/ Cerebral hemorrhage • Status Epilepticus • Typhoid fever • Catatonia
Amphetamines • Used and abused since 1930’s after reports of enhanced intellectual performance. • Schedule I: MDMA (ecstasy), MDA, MDEA • Schedule II: Adderall, Ritalin, etc. • OTC: Ma Huang (ephedra), Sudafed
Amphetamines • Mechanism: Enter neurons via serotonin/dopamine transporters, displace storage vesicles leading to NE, serotonin, and dopamine efflux. • Catacholamine release leads to tachycardia, inc SVR, mydriasis, and hyperthermia.
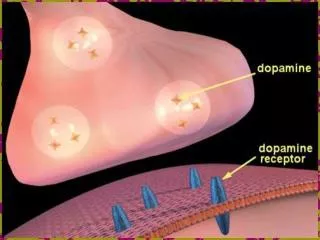
Amphetamine increases the concentration of dopamine in the synaptic cleft in 3 ways: • (1) bind to the pre-synaptic membrane of dopaminergic neurones and induce the release of dopamine from the nerve terminal • (2) interact with dopamine containing synaptic vesicles, releasing free dopamine into the nerve terminal • (3) bind to the dopamine re-uptake transporter, causing it to act in reverse and transport free dopamine out of the nerve terminal. Amphetamine can also cause an increased release of noradrenaline into the synaptic cleft.
Acute Toxicity • May present w/ AMS, agitation, seizures, palpatations, chest pain, n/v/d. • Severe Hyperpyrexia • Hyponatremia • Secondary Conditions: • Rhabdomyolysis • DIC • Renal Failure • Hepatic Necrosis • GI Bleeding • Diarrhea
Acute Toxicity • Thermoregulatory: up to 43 deg, which leads to rhabdo, DIC, multiorgan failure • CV: tachy, inc SVR, HTN, dysrhythmia, late- hypotension • Neuro: stimulant effects to coma • Electrolyte: Severe hyponatremia, acidosis and rhabdo changes • GI: Hepatotoxicity and GI Bleeding • MSK: rhabdomyolysis • Renal: ARF from rhabdo, DIC, shock • Heme: DIC
Chronic Toxicity • Risk of vasculitis • Neuropsychiatric abnormalities • Damage to dopaminergic and serotonergic neurons • Cardiomyopathy
Learning Points • 1. Hyperthermia has a broad differential, and drugs of abuse should be kept in mind. • 2. Watch for rhabdomyolysis, DIC, and multiorgan failure after hyperpyrexia. • 3. Amphetamines result in dopamine, NE, and serotonin release, catecholamine surge!
Sources • White, S. Amphetamine Toxicity. Seminars in Resp & Critical Care Medicine Vol 23, 2002. • Lanken, PN. UpToDate. Hyperthermia. 2008. • Stahl S. Drugs of abuse. Essential Psychopharmacology – neuroscientific basis and practical applications. Cambridge University Press: Cambridge. 1996:332–366.