Download
1 / 34
340 likes | 474 Views
What’s New in Nutrition?. NJ Maxvold MD Associate Professor of Pediatrics Pediatric Critical Care Medicine DeVos Children’s Hospital. Nutrition and PCRRT. Is there anything New? Current General Knowledge: Stress Response elicits change in Utilization of Fuel/Substrates:

E N D
What’s New in Nutrition? NJ Maxvold MD Associate Professor of Pediatrics Pediatric Critical Care Medicine DeVos Children’s Hospital
Nutrition and PCRRT Is there anything New? Current General Knowledge: Stress Response elicits change in Utilization of Fuel/Substrates: • Cellular (End Organ) Insulin Resistance, therefore hyperglycemia and altered cellular energetics • Fatty Acids increased utilization as Glucose Utilization becomes Inefficient • Protein metabolism shift from anabolism to catabolism • Phasic changes in metabolism during acute Illness
Nutrition and PCRRT Carbohydrate Utilization • Limit of oxidation of Carbohydrate ~ 5 mg/kg/min of Glucose • Hyperglycemia Insulin Resistance Gluconeogenesis
Nutrition and PCRRT Lipid Metabolism Fatty Acid Utilization (major myocardial oxidation fuel) Mitochondrial adaptation to acute stress (Carnitine dependent enzymes) Calvani et al Basic Res Cardiol 2000 Mitochondrial control of FFA oxidation and CHO oxidation AcetylCoA/ CoA ratio on PDH Complex
Nutrition and PCRRT High Protein Catabolism • Muscle Efflux of Amino Acids to fuel Gluconeogenesis • Protein metabolism shift from anabolic to Acute phase proteins (Hepatic Inflammatory Response) Net Negative Nitrogen Balance
Critical Illness • hormone changes • Acute: increase • Later: decrease ↑ cytokines Altered substrate utilization CHO: ↑hepatic gluconeogenesis (shift away from liver glycolysis) Hyperglycemia - Inefficient glucose oxidation - Insulin resistance - Shift in use of amino acids: gluconeogenesis + APR’s MALNUTRITION Impaired nutrient transport Inefficient/inadequate supply Impaired A.a. conversion ↓lipid oxidation Uremia Acidosis Altered Glucose metab. Cytokines Acute Kidney Injury
Nutrition and PCRRT Impaired Nutrient Support: Diminished Cellular Energy • Inefficiency of normal cellular transport activities: • Disturbances in the Na/K ATPase pump (energy dependent function) • Intracellular mitochondrial adaptations (Dysfunctional electron transport respiration) Muscle wasting & Malnutrition h Mortality
Nutrition and PCRRT Adequate Calories: REE or Indirect Calorimetry ??Should we add 10-15 % or More?? REE in Children : 35-60 kcal/kg/d Briassoulis et al Crit Care Med 2000 MEE in Crit Ill Children: 30-35 kcal/kg/d ?? How soon?? Heyland D et al JPEN 2003 24-48 Hrs
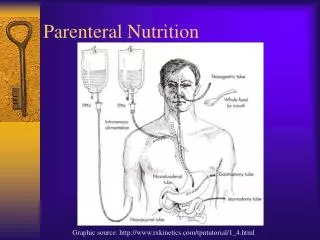
Indirect calorimetry AND CRRT • IC: measure resting energy expenditure. • Based on: Expired CO2 and O2 (O2 consumption + CO2 production). Potential problem with CRRT May affect IC measurements. IC may not be reliable? HCO3/CO2 fluxes Hemofilter Effluent Dialysis fluid
Nutrition and PCRRT • Protein Support for Nitrogen Balance: • Nitrogen Intake = Nitrogen Output Protein Catabolic Rate in AKI: Macias et al JPEN 1996 ~ 1.4 -1.7 g/kg/day Maxvold et al Crit Care Med 2000 ~ 1.2 - 1.8 g/kg/day
Nutrition and PCRRT Can Nitrogen Balance be Achieved in AKI patients on CRRT? Conflicting Studies Bellomo et al Ren Fail 1997 Protein Intake : Nitrogen Balance 1.2 g/kg/d AA -5.5 g N /d 2.5 g/kg/d AA -1.9 g N /d
Does Increasing Protein Intake Help? Scheinkestel et al Nutrition 2003 • 11 critically ill adults on CRRT, protein intake 2.5 g/kg/day a) normal amino acid levels b) positive nitrogen balance. • 50 critically ill adults on CRRT: 1.5 vs 2.0 vs 2.5 g/kg/day. NB related to protein intake. NB related to hospital stay Protein intake 2.5 g/kg/d: improved survival!
Protein intake (g/kg/day) Day of CRRT Protein and calorie prescription for children and young adults receiving CRRT: a report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry group. Zappitelli et al, submitted. Daily change in protein prescription during treatment with CRRT.
Protein and calorie prescription for children and young adults receiving CRRT: a report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry group. Zappitelli et al, submitted. • All groups: • Maximal protein>initial • Multivariate predictors of • maximal protein intake • Younger age • Higher initial protein Rx • #CRRT days Protein Rx >2g/kg/day in 40%
Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted Protein and energy intake and output at CVVHD1 initiation, Day 2 and Day 5. Maxvold et al, Crit Care Med, 2000 Protein intake was 1.5 g/kg/day – Negative nitrogen balance It’s not easy to achieve a positive nitrogen balance. Logic: bigger filter, higher Qd or Quf = increased clearance
Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted CVVHD clearance of amino acids measured on Day 2 and Day 5 N=15
Combined results of clearance of essential amino acids by CRRT. Zappitelli et al (submitted) and Maxvold et al, Critical Care, 2000 (n=6). Several studies, adult and child: ~ 10-20% intake “lost” through hemofilter. Both studies: Highest losses with Glutamine/Glutamic acid
Critical Illness – trace metals • Deficiencies linked to: • Lymphocyte dysfunction • Cardiovascular dysfunction • Platelet activity • Antioxidant function • Wound healing
Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted Churchwell et al, NDT, 2007 Critically ill adults receiving CVVHD and CVVHDF Transmembrane clearances Much lower clearance of selenium and chromium Overall, trace metal clearance negligible.
CRRT-Vitamins Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted * *
Nutrition and PCRRT Berger et al AM J Clin Nutr 2004 24º Balance Studies Intake(Replacement Fluid) = Output (Effluent) [SeRF] = [SeEff] -0.97 µmol (2 x RI) [CuRF] = [CuEff] -0.54 µmol (0.3 x RI) [Vit B1RF] = [Vit B1Eff] -4.12 mg (1.5 x RI) [ZnRF] = [ZnEff] 20.7 µmol (1.5 x RI) Negative Balance for Se, Cu, VitB1 and Se and VitB1 Losses > 1.5 x the Recommended Intake
Critical Illness - Vitamins Water Soluble • Vit B1 Def Altered Energy Metabolism, h Lactic Acid, Tubular damage • Vit B6 Def Altered Amino acid and lipid metabolism • Folate Def Anemia • Vit C Def Limit 200 mg/d as precursor to Oxalic acid Potential for losses during CRRT.
Critical Illness - Vitamins Fat Soluble • Vit D Def Hypocalcemia • Vit A Excess i renal catabolism of retinol binding protein • Vit E Def i >50% plasma and RBC
Critical Illness & AKI - Lipids • h LDL and VLDL • iCholesterol and HDL-Cholesterol Impaired Lipolysis Lipase Activity ~50% iLipoprotein Lipase i Hepatic Triglyceride Lipase
Nutrition and PCRRT Initial Nutritional Prescription for Kids with AKI on CRRT: • Early Nutrition : 24-48 hrs of PICU admission • Enteral feeding + Parenteral feeding (often require partial Parenteral Nutrition early in acute illness) • REE for age (without additional kcal % allowance) ( REE is already >33% Above mean MEE ) • MEE if available
Nutrition and PCRRT Future Development PharmacoNutrients: • Gln • Omega 3 Fatty Acids • Arginine • L-Carnitine • Growth Factors
PharmacoNutrients Singer et al Intensive Care Med 2008 • Omega-3 FA: Augment immune defense through inhibition of NF-kappaß Luiking st al Crit Care Med 2007 Kalil et al Crit Care Med 2006 • Arginine: + Effect - Improved microcircuation, gut function, Plt and WBC Adherence,Endothelial function - Effect -Hemodynamic Instability, Oxidative Stress Prevotet al Pediatr Nephrol 2009 • Growth Factors(IGF-1, GH, Insulin)
Glutamine: Conditionally Essential Nutrient • Substrate for Rapidly dividing cells(Kidney tubular cells, Enterocytes, Immune cells) • Precursor for Glutathione • Substrate for Gluconeogenesis • Substrate for Ammoniagenesis • Osmotic regulator, • Precursor of purine/pyridimine
Potential Beneficial Effects of Glutamine Enhanced Heat Shock Protein GLN Pool Enhanced insulin sensitivity Decreased Free Radical availability (Anti-inflammatory action) Inflammatory Cytokine Attenuation Glutathione Synthesis Glutamine Therapy Reduced Translocation Enteric Bacteria or Endotoxins Maintenance of Intestinal Mucosal Barrier Fuel for Enterocytes Critical Illness Nuclotide Synthesis Preservation of TCA Function Reduction of Infectious complications Maintenance of Lymphocyte Function Fuel for Lymphocytes Anti-catabolic effect Preserved Cellular Energetics- ATP content Preservation of Muscle mass GLN pool
Glutamine Studies • CRISIS Trial: Multicenter Pediatric Trial of Enteral Se, Zn, Gln, IV Metoclopramide 1º Outcome: Time between PICU [DOA] and Infection [nosocomial or clinical] • REDOXS Study: Multicenter Adult Trial 4 Treatment Arms: Gln; Gln and AntiOxidants; Antioxidants; Placebo Remember! Gln Loss on CRRT:15-20% of Total AA Clearance
Nutrition and PCRRT Carnitine Studies • Conditionally Essential Supplement • Improved Mitochondrial Cellular Energetics
Nutrition in PCRRT Carnitine Role in Cell Energetics: • Facilitates Long Chain AcylCoA [transformed FattyAcids within cytosol] • Diminishes Acetyl CoA/CoA Ratio - Improves the PDH Complex Activity • Increases Pyruvate Oxidation and decreases Lactate Production
Nutrition in PCRRT That’s Enough for Now! Many Thanks and Gratitude : Dr. Bunchman Dr. Zappitelli My Associates in Michigan, especially the PICU nurses!