Download
1 / 12
120 likes | 686 Views
Epidemiology of Uveitis. Incidence and Prevalence of Scleritis and Episcleritis In Veterans Affairs Medical Centers of the Pacific Northwest. ASCRS 2008 - Chicago Michael Lloyd, MD, Eric B. Suhler, MD, MPH Dept of Ophthalmology, Portland VA Medical Center

E N D
Epidemiology of Uveitis Incidence and Prevalence of Scleritis and Episcleritis In Veterans Affairs Medical Centers of the Pacific Northwest ASCRS 2008 - Chicago Michael Lloyd, MD, Eric B. Suhler, MD, MPH Dept of Ophthalmology, Portland VA Medical Center Casey Eye Institute, OHSU, Portland Oregon
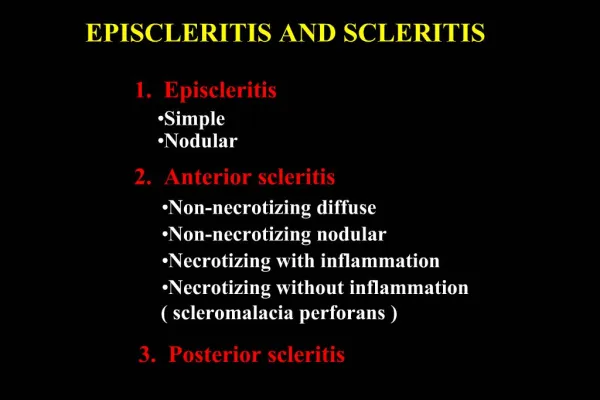
Introduction • Epidemiology is the study of factors • leading to disease in populations. It serves as • the foundation and logic of interventions made in the interest of public health. • Although rare, scleritis is a significant public health problem because: • It can be the presenting sign of life- and sight-threatening disease • it is associated with high rates of vision loss (9% with diffuse, 26% with nodular, 74% with necrotizing, and 84% with posterior scleritis) • -30% of people with necrotizing scleritis will be dead within 8 years of presentation without treatment
Introduction There is nopopulation-based literature on the epidemiology of scleritis, but a few referral-based studies exist Williamson 1974 – 8 years at Southern General Hospital in Glasgow 8 scleritis cases out of 9600 new referrals Watson and Hayreh 1976 – 10 years at Moorfields 207 episcleritis and 159 scleritis cases in 10 years of a special scleritis clinic Foster 1993 – 11 years at Mass Eye and Ear 94 episcleritis and 172 scleritis cases out of 6600 new referrals
Methods We sought to ascertain the incidence and prevalence of scleritisvia by a large, population-based study using the VA centralized database (CHIPS) as our model We searched for any encounter within FY04 coded for scleritis or episcleritis at any VAMC in Oregon or Washington state Each case was independently reviewed by an ophthalmologist using standardized criteria to document location, onset, continuity, laterality, and associated diagnoses according to the SUN criteria Jabs et al, AJO 1995 Questionable cases were reviewed by a second ophthalmologist specializing in uveitis
Methods Scleritis cases had to have some combination of pain, scleral injection, edema, or thinning. Episcleritis cases required episcleral injection and discomfort and could not be associated with discharge.
Methods A case that had active disease which was well controlled with medication would be included as prevalent Cases with documented inflammation in the past, but no current therapy or inflammation during the study period were classified as “inactive prevalent” and not included in the calculations Cases with inadequate documentation in any area were classified as “indeterminate” and not included in the calculations
Results Total population surveyed – 152,267 Cases with ICD9 codes reviewed - 519 Incident scleritis cases in FY04 – 2 (1.3 cases/100,000 person-years) Prevalent scleritis cases in FY04 – 12 (7.88 cases/100,000 population) Incident episcleritis cases in FY04 – 12 (7.22 cases/100,000 person-years) Prevalent episcleritis cases in FY04 – 19 (12.48 cases/100,000 population)
Results Cases by age group and gender Scleritis – average age 61 Episcleritis – average age 54
Results Number of associated disorders *not known to be reported as associated with scleritis
Discussion This is the first population-based study to describe the epidemiology of scleritis and episcleritis There are some weaknesses in our study -difficulty in diagnosing episcleritis second hand - still likely to underestimate episcleritis cases -homogeneous population does not reflect the wider public health (elderly white men are over- represented) -documentation was insufficient to further classify cases into diffuse, nodular, necrotizing, etc
Discussion Our data confirm the behavior of scleritis and episcleritis as two different disorders. -Although rare, scleritis tends to be more chronic and is much more likely to be associated with a systemic autoimmune disorder (50% of cases) -Episcleritis is more common, but shorter-lived; no “progression” was noted from episcleritis to scleritis - Likely more frequent in women; more frequent in the 45-65 age group with scleritis occurring in a slightly older population
References Watson PG, Young RD. Scleral Structure, organisation, and disease. A review. Experimental Eye Research. 2004. 78:609-623. Pavesio CE, Meier FM. Systemic disorders associated with episcleritis and scleritis. Current Opinion in Ophthalmology 2001. 12:471-478 Albini TA, Rao NA, Smith RE. The Diagnosis and Management of Anterior Scleritis. International Ophthalmology Clinics. 2005. 45(2):191-204. Watson PG, Hayreh SS. Scleritis and episcleritis. British Journal of Ophthalmology. 1976. 60:163-191 Okhravi N, Odufua B, McCluskey P, Lighman S. Scleritis. Survey of Ophthalmology. 2005. 50(4):351-363. McCluskey PJ, Watson PG, LIghtman S, et al. Posterior scleritis: clinical features, systemic associations, and outcome in a large series of patients. Ophthalmology. 1999. 106:2380-6. Jabs DA, Mundun A, Dunn JP. Episcleritis and Scleritis: clinical features and treatment results. American Journal of Ophthalmology 2000. 130:469-76. Williamson J. Incidence of eye disease in cases of connective tissue disease. Transactions of the ophthalmological societies of the United Kingdom. 1974. 94 (3):742-52. Watson PG, Tuft SJ. Progression of Scleral Disease. Ophthalmology 1991. 98(4): 467-71. Watson PG, Hazleman BL, Pavesio CR, Green WR. The Sclera and Systemic Disorders Second Edition. Butterworth Heinemann. London. 2004. Foster CS, Sainz de la Maza, M. The Sclera. Springer-Verlag. New York. 1994.