Download
1 / 26
260 likes | 288 Views
Learn how Bone Mineral Density (BMD) testing aids in diagnosing osteoporosis, assessing fracture risk, monitoring changes, and guiding treatment. Understand guidelines, techniques, and strategies for fracture prevention with BMD measurements.

E N D
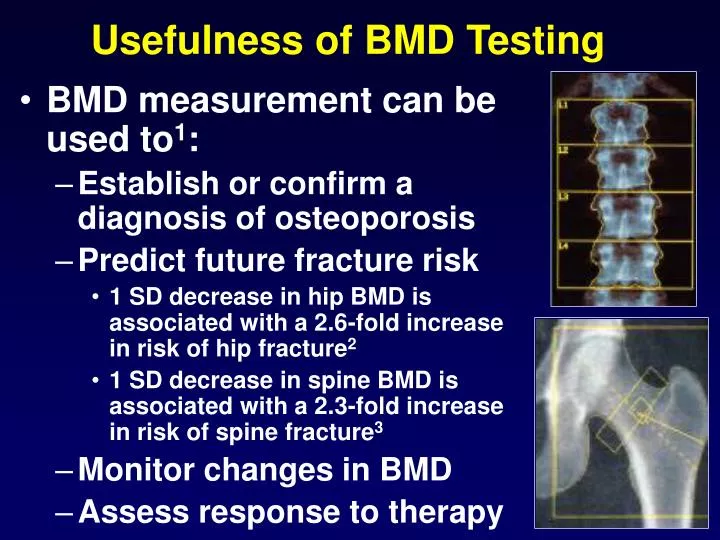
Usefulness of BMD Testing • BMD measurement can be used to1: • Establish or confirm a diagnosis of osteoporosis • Predict future fracture risk • 1 SD decrease in hip BMD is associated with a 2.6-fold increase in risk of hip fracture2 • 1 SD decrease in spine BMD is associated with a 2.3-fold increase in risk of spine fracture3 • Monitor changes in BMD • Assess response to therapy
Guidelines for BMD Measurements in Postmenopausal women : NOF • BMD testing only if results likely to influence Treatment decisions BMD Testing: • All women age 65+ • Women <65 with Risk factors ( Parental History of Fx, smoking, weight <57.2 kg, use of oral corticosteroids >3 mos, conditions 2o osteoporosis • Women with Fracture after age 45
Guidelines for BMD Measurements in Postmenopausal women : USPSTF BMD Testing: • All women age 65+ • Women age 60-64: with Risk factors ( Parental History of Fx, smoking, weight <57.2 kg, use of oral corticosteroids >3 mos, conditions 2o osteoporosis) • No Recommendations for or against routine screening in women < age 60
Summary Of Common Techniques for assessment of Bone Mass SITE Scan time Prec- Radiation Cost min ision(%) mrem $ Peripheral Radius, calcaneous 5-15 1-3 1 40 Central spine,hip, body 5-10 1-2 1-5 128 QCT Spine 10-30 2-4 50 185 RA Hands 5-10 1-2 5 38 QUS Calcaneous,tibia 5-10 3-4 0 53 DXA
Low bone mass Smoking Impaired visual function Long acting sedatives High caffeine / low calcium Physical activity Muscle weakness Poor health Low body weight Weight loss History of falls Little / no sunlight exposure Parkinson’s disease Low Estrogen Age Family history Gender Race Tall (young adult) Late menarche Impaired mental status Longer hip axis length Summary: Risk Fractures for Hip Fracture Potentially Modifiable Unmodifiable
Annual Risk of Hip Fracture According to the Number of Risk Factors and Age-Specific Calcaneal Bone Density Rate of Hip Fracture (per 1000 women-yrs) # of Risk Factors Calcaneal BMD Tertile
What is Our Desired Outcome in Osteoporosis? Fractures are the cause of osteoporosis morbidity and mortality! Fracture Reduction
Conclusions • Maximize Peak Skeletal Mass • Prevent or Slow-down Rates of Bone Loss • Prevent Falls Key is Prevention
Enhance the Development of Peak Bone Mass • Proper Nutrition • Exercise • Avoidance of Premenopausal Estrogen Deficiency • No Smoking or Excessive Alcohol • Subgroups at High Risk (cystic fibrosis, ?asthma, IBD, celiac, Hypo-gonadism, anorexia)
Strategies to Reduce Fracture Incidence • Population Approach • Influence the Overall Distribution of BMD • Adequate dietary calcium: 1200 mg/day • Vitamin D: 400 to 800 IU • Exercise • Stop smoking
Strategies to Reduce Fracture Incidence • Treat modifiable risk factors • Unmodifiable risk factors • Identify women who will benefit from treatment Individual Approach
Effect of Dosage and Timing: Two Participants Taking 2000 mg Calcium Dose % Absorption Calculation #1 2000 mg 14% 2000 X 0.14 = 280 Total = 280 mg Ca #2 500 mg 29% 500 X 0.29 = 145 500 mg 29% 500 X 0.29 = 145 500 mg 29% 500 X 0.29 = 145 500 mg 29% 500 X 0.29 = 145 Total = 580 mg Ca
Resistance exercise • Lack of resistance (immobilization or lack of gravity) clearly leads to bone loss. • BMD preservation ~ or modest increase ~ found in many but not all studies • Strength, flexibility, mobility, balance may also help prevent falls
Prevention of Falls • Exercise and physical activity • Rehabilitative therapies: balance and gait training • Medications • Environmental and Behaviorial interventions • Multiple Risk Factor Interventions
Risk Factors for Fracture: Recommendation for Treatment • Low BMD • History of prior fracture after age 40 • History of fracture at the hip, wrist or vertebra in a first degree relative • Being in lowest quartile of body weight < 57.8 kg • Current cigarette smoking Osteoporosis Int 1998:8(S4):16.
The 2001 NIH Consensus Panel: • “There is not yet good evidence to support the efficacy of early initiation of preventive drugs…”
The sample size needed to prove fracture prevention in young women is enormous vertebral fractures B M D child/teens 35 50 60 70 hip fractures rapid postmenopausal loss 1-5%/year
Approved drugs for Prevention Approved drugs for Treatment Estrogen Raloxifene Alendronate Risedronate Alendronate Risedronate Raloxifene Calcitonin Estrogen Risedronate
ESTROGEN RALOXIFENE BISPHOSPHONATES MECHANISM OF ACTION OF ANTI RESORPTIVE DRUGS BONE RESORPTION OSTEOCLAST PRECURSORS INACTIVE OSTEOCLAST ACTIVE OSTEOCLAST
6 6 4 4 2 2 0 0 –2 –2 –4 –4 –6 –6 HRT: Effect on BMDPostmenopausal Estrogen/Progestin Interventions Trial (PEPI) Spine Hip Percent Change from Baseline Baseline 12 mo 36 mo Baseline 12 mo 36 mo Placebo CEE Only CEE-MPA (cyc) CEE-MPA (con) CEE-MP (cyc)
Clinical Outcomes (Annualized %) by Randomization Assignment HR 95% CIEstrogen+Progestin Placebo Nominal Adjusted Hip fractur e44 (0.10%) 62(0.15%) 0.66 (0.45-0.98) (0.33-1.33) Vertebral 41 (0.09%) 60 (0.15%) 0.66 (0.44-0.98) (0.32-1.34) 579 (1.31%) 701 (1.70%) 0.77 (0.69-0.86) (0.63-0.94)fracture* Total fracture 650 (1.47%) 788 (1.91%) 0.76 (0.69-0.85) (0.63-0.92) *Other osteoporotic fractures include all fractures other than chest/sternum, skull/face, fingers, toes and cervical vertebrae, and hip and vertebral fractures (reported separately).
Can low dose estrogen prevent bone loss? Change (%) in Spinal BMD • RCT, n=128; >age 65 • Low bone mass (t-score < -1.4) • Calcium 1000 mg/day • Serum Vitamin D (25-OH): 75 nmol/L • CEE (0.3 mg/day) and MPA (2.5 mg/day) • Follow-up 3.5 years
WHI Estrogen+Progestin TrialImplications • Estrogen plus progestin should not be initiated or continued for the primary prevention of chronic disease in healthy women • The risks for CHD, stroke, PE and breast cancer must be weighed against the benefit for fracture in selecting from the available agents to prevent osteoporosis