Download
1 / 22
250 likes | 559 Views
Glomus jugular tumor. Chunfu Dai M.D & Ph.D. Background. Originate from chemoreceptor jugular vein glomus jugulare tumor is arisen in the adventitia of the dome of the jugular bulb This tumor is part of the neuroendocrine system, these tumors are highly vascularized.

E N D
Glomus jugular tumor Chunfu Dai M.D & Ph.D
Background • Originate from chemoreceptor jugular vein • glomus jugulare tumor is arisen in the adventitia of the dome of the jugular bulb • This tumor is part of the neuroendocrine system, these tumors are highly vascularized. • Glomus tumors represent 0.6% of neoplasms of the head and neck
Pathology All paraganglia are composed of chief cells (type I cells, ie, chemoreceptive cells) and sustentacular cells (type II cells, ie, supporting cells). Developmentally, both types of cells are of neuroectodermal origin; specifically, they arise from neural crest cells The vast majority of glomus tumors are benign and slow to grow with bone erosion.
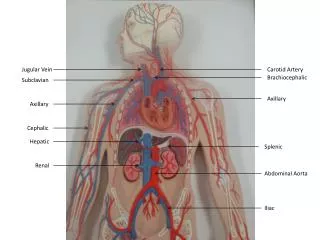
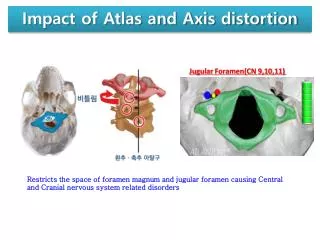
Pathology • Glomus jugulare tumors are typically located just under the skull base, at the bulb of the internal jugular vein. The tumors may spread superiorly into the jugular foramen, causing CN IX, CN X, and CN XI deficits. • The primary blood supply to jugulare tumors is via the ascending pharyngeal artery. In addition, the occipital and posterior auricular arteries can contribute to vascularization. • Intraoperatively ligation of external carotid artery can significantly reduce the hemorrhage
Symptoms • Pulsatile tinnitus, • Conductive hearing loss, aural bleeding, and aural discharge. • Sensorineural hearing loss, vertigo, aural pain and • Cranial neuropathy. Such as it can compress CN IX, X, and XI.
Symptoms • Functioning tumors, which are rare, can increase risk of mortality. These active tumors secrete catecholamines, which can lead to clinical manifestations of hypertension, headaches, palpitations, and tachycardia
Signs • Positive Brown’s sign. • Aural polyp • Cranial nerves involvement
Lab tests • Routine laboratory studies are not helpful • In the rare patient with functioning lesions, preoperative and postoperative catecholamine measures may help confirm successful resection of the lesion
Image study • A combination of contrast-enhanced CT, MRI, and angiography is ideal for proper diagnosis and localization of the tumors. • MRI • Contrast-enhanced CT • Angiography remains of paramount importance if the diagnosis is obscure or if embolization is planed.
CT • Glomus jugulare tumors are enhancing soft-tissue masses at the skull base, but skull-base artifact can mask their presence. • These tumors are seen within the jugular foramen. • The demonstration of bone erosion of the jugular foramen and petrous apex is often a key finding in the diagnosis. Careful review of bone windows is necessary.
MRI • It can show intense tumor enhancement, and is a key finding in the diagnosis. • A salt-and-pepper fine vascular pattern can be seen in the tumors; this finding is suggestive of intrinsic tumor neovascularity, particularly on T2-weighted images.
MRI • Images show that enhancing soft-tissue masses protrude both intracranially and extracranially at the skull base. Coronal imaging can show tumoral relationships to the brainstem and skull base, and deep cervical soft-tissue structures
AG • Demonstrating the feeding artery • Jugulare tumors involve higher external carotid branch vessels; the ascending pharyngeal, tympanic, and occipital arteries dominate the arterial blood supply. • Arteriovenous fistulae may be present. • Rarely, the internal carotid and vertebral arteries may contribute feeders to the neoplasms. • Typically, these tumors are evaluated, with attention paid to all potential feeding arteries.
Contraindication • Biopsy is prohibitive for patient with glomus jugular tumor • Due potential hemorrhage
Surgical Intervention • Surgery is the preferred method of treatment for glomus tumors. • Most paragangliomas are slow-growing and benign, radiotherapy alone or no treatment at all is preferred in elderly patients in whom the risks of surgery are relatively high and the tumor is unlikely to cause serious morbidity or mortality. • If the patient is young, surgery is the best option that allows total cure.
Surgical Intervention • Current techniques are highly successful with relatively low morbidity rates: Blood loss and CN neuropathies are the major complications. • Depending on the specific type and location of the tumor, different surgical approaches are required.
Surgical Intervention • Extensive facial recess approach
Surgical Intervention • Mastoid –neck approach: • tumors are confined to jugular foramen and may extend to the middle ear and mastoid. They do not involve the carotid artery or the intracranial compartment. • Infratemporal fossa approach: • tumors involve in carotid artery and transdural tumor are far more extensive.
Radiotherapy • Gamma-knife irradiation is used in patients who are poor candidates for surgical excision or embolization due to their age or disease state or because of unacceptable morbidity. • This procedure is expensive, and clear remission is not reported. • It can control the tumor and prevent it from growing larger.
Embolization • Embolization is a common technique used as the lone treatment option or as a precursor to surgical excision. • Starving the lesion of its blood supply and inducing necrosis.. • embolization is often used to reduce blood loss, and it has been proven to be highly effective. • Care must be taken to avoid inadvertent extracranial-intracranial embolization and the subsequent the risk of stroke
Thanks for your attention