Download
1 / 19
190 likes | 202 Views
Linking EHRs Between PH, Social Service Agencies, and Other Relevant Organizations. How to Create Information Systems With Data that Flow Both Ways. Arthur Davidson, MD, MSPH Denver Public Health adavidson@dhha.org

E N D
Linking EHRs Between PH, Social Service Agencies, and Other Relevant Organizations How to Create Information Systems With Data that Flow Both Ways Arthur Davidson, MD, MSPH Denver Public Health adavidson@dhha.org Committee on Recommended Social and Behavioral Domains and Measures for Electronic Health Records National Academies of Sciences Building 2101 Constitution Avenue NW Washington, DC 20418 April 8, 2014
Agenda • Conceptual Model • Linkage for Public Health Surveillance • Linkage for Public Health Intervention • Next Steps
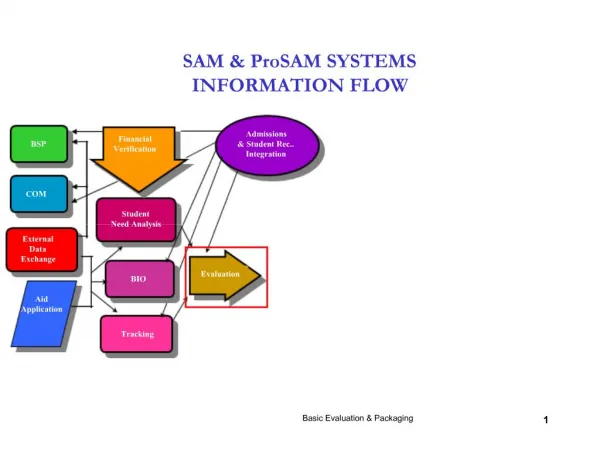
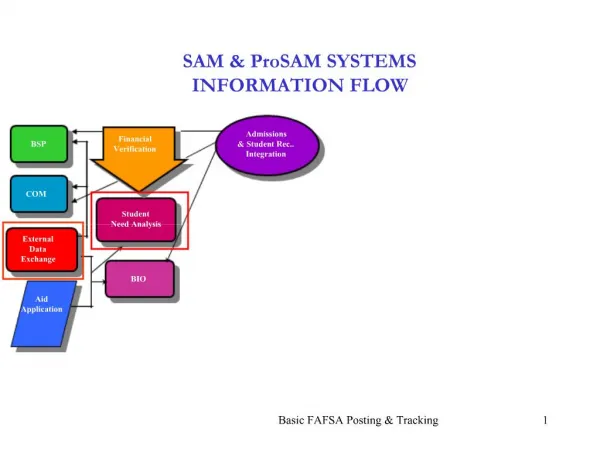
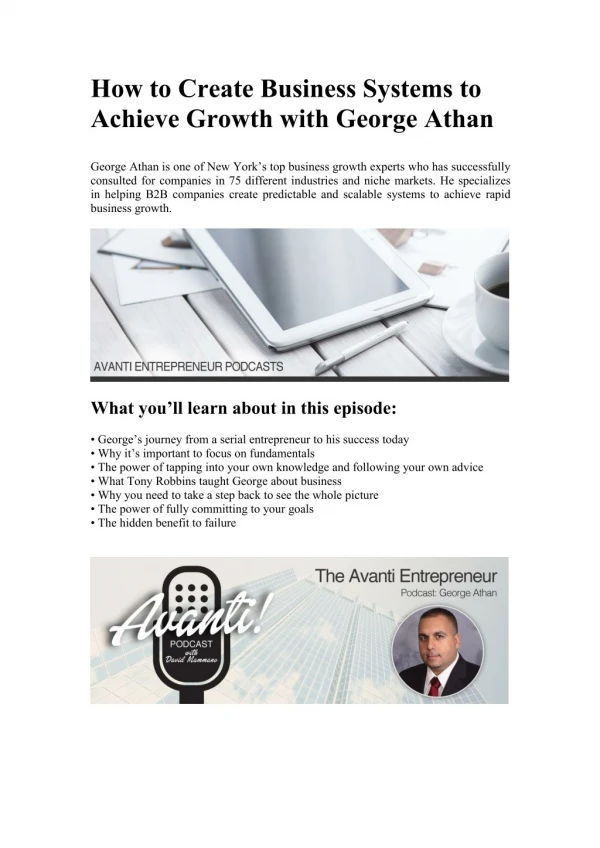
Linkage Conceptual Model Quitline Social Service Clinical Care (EHR) Public Health Schools/Childcare
Linkage for Public Health Surveillance(Colorado) • Transparent, distributed data network • Modeled on the Mini-Sentinel (FDA) project and local experience with HMO Research Network (AHRQ) project • Governance • Voluntary participation; unlike mandated reporting, data use agreements established/required • Privacy • Minimal data necessary to achieve stated goal (de-identified to start) • Technical • Infrastructure: 1) common data model, 2) emphasize data quality assessment, and 3) federated query tool
Linkage for Public Health Surveillance(Colorado) • Colorado Health Observation Regional Data Service (CHORDS) • Provide a "laboratory" to develop and evaluate scientific methods to support public health surveillance • Afford Denver Metro and Colorado communities an opportunity to use existing EHR data systems for public health surveillance • Learn about barriers and challenges, both internal and external, to building a viable and accurate system of surveillance for public health events (e.g., conditions, behaviors and outcomes) • Build an event agnostic infrastructure for public health surveillance, quality assessment, and research
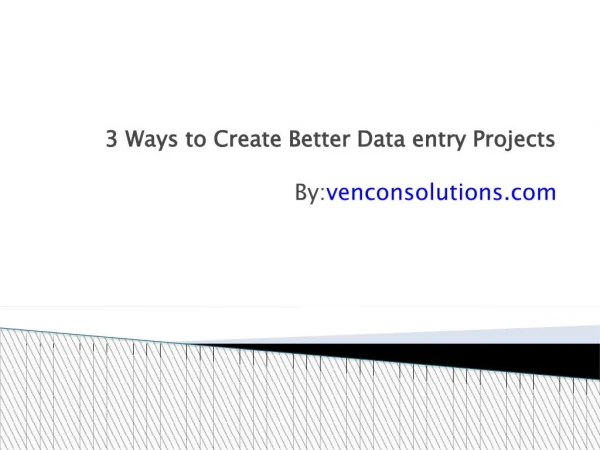
CHORDS RegistriesColorado Health Observation Regional Data Service e.g., Kaiser Permanente Standard (Virtual) Data Warehouse • Current registry efforts: • BMI • CVD risk • Tobacco use and SHS exposure • Mental health • Colorectal cancer • Adult obesity PMN Client Secure federated query CHORDS Query Service (PopMedNet ) PMN Authorize Authenticate e.g., Denver Health Standard (Virtual) Data Warehouse Secure federated query PMN Client
Link Clinical, Social and Environmental Data Across Multiple Delivery Systems Pre-CHORDS (e.g., weight status surveillance): • BRFSS self-reported demographic, weight data • Survey ~12,000 Colorado/year = 700 Denver/year • Allows county-level estimates only CHORDS state: • Combine measuredBMI data from multiple institutions • Include demographic data, residence location (geo-code) • Link geographically aggregated BMI data (e.g. census tract) with social and environmental data • Identify “place-based” interventions (e.g., social marketing, community resource development, and policy initiatives) • Pilot features of local data sharing network
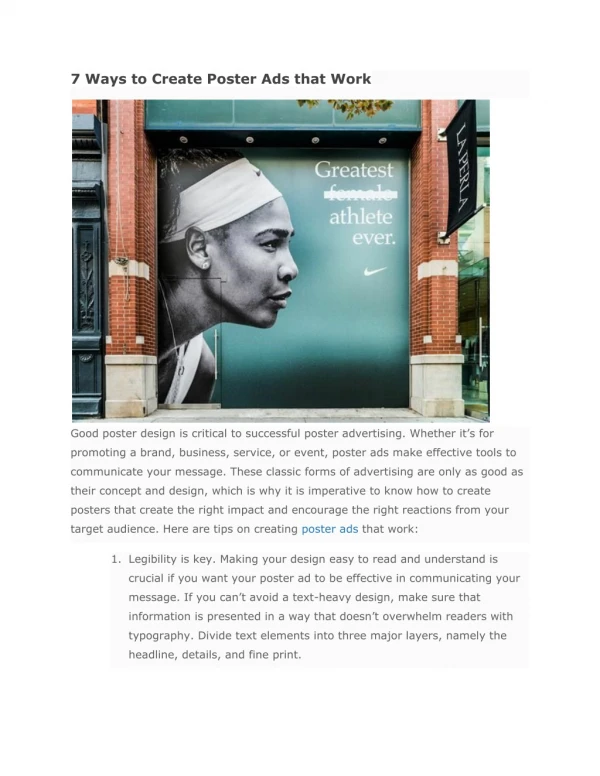
Types and Sources of Geo-coded Social and Environmental Data for Mapping
Combined Measured BMI Data • Denver County (valid BMI) : • all ages: 184,644 (31%) • adults: 119,075 (26%) • children: 64,606 (51%) • Coverage varies widely: • > 50% for some communities • few with aberrant results
Linkage Conceptual Model Quitline Social Service Clinical Care (EHR) Public Health Schools/Childcare
e-Referral between EHR and Quitline Goal: Efficient EHR-mediated e-Referral (including patient preferences) to Quitline and timely acknowledgement/status messages returned to and posted within the EHR. • North American Quitline Consortium • Consensus process with ~15 Quitlinevendors/service providers • Message requirements: • Content: define common data elements • Structure: HL7 2.x and c-CDA formats • Transport: sFTP, Direct, web-service (WSDL-SOAP)
What next? CHORDS • Build out standard data model (i.e., add tables, required content/variables [IZ], extend time range) • Conduct comprehensive data quality assessment • Compare member-vs. visit-based denominator estimates • Expand stakeholders (PH and clinical) • Address duplicates Quitline • Set e-Referral standards, assure meets PH needs • Vet with EHRA and standards development organization • Consider as model for PH related HIE and e-referral for other community-based services
Sustainability strategy • Enhance “event agnostic” distributed surveillance/research network (e.g., breadth of use cases and stakeholders, depth of content) • Study utility of system to multiple stakeholders (i.e., communities, elected officials, and individuals) • Facilitate incorporation of new social/environmental data (e.g., barriers and assets) • Standardize approach to geocoding and de-duplication • Target outreach and community-based interventions (i.e., policy, systems and environmental changes) to those who need them • Assess impact on health disparities reduction • Develop cadre of applied researchers and methods