Download
1 / 15
160 likes | 355 Views
Patient specific QC in Aarhus. Lone Hoffmann Ulrik Vindelev Elstrøm, Mai-Britt Kyed Jørgensen. VMAT introduction. Introduced in May 2009 First patient: June the 17th, 2009 Treated approx. 800 patients Primarily pelvic cancers Prostate, cervix, bladder, anal, rectum,.. Other types:

E N D
Patient specific QC in Aarhus Lone Hoffmann Ulrik Vindelev Elstrøm, Mai-Britt Kyed Jørgensen
VMAT introduction • Introduced in May 2009 • First patient: June the 17th, 2009 • Treated approx. 800 patients • Primarily pelvic cancers • Prostate, cervix, bladder, anal, rectum,.. • Other types: • Brain, sarcomas, abdominal
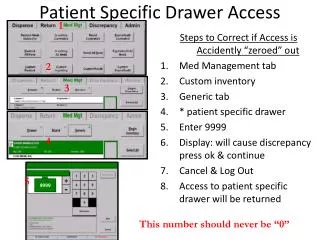
Patient specific QA • Perform Delta4 verification for all patients • Normalization to daily output • Gamma(3,3) > 95 % • Most patients: G(3,3) > 97 %
Test/learning plans • 10 prostate plans (15MV)were created with: • 250MU, 500MU, 750Mu, 1000MU, 2000MU • In 1 or 2 arcs • 10 H&N plans (6MV) were created with: • 250MU, 500MU, 750Mu, 1000MU, 2000MU • In 1 or 2 arcs • 2 Gy/fx
G(3,3) vs. #MUs • G(3,3) decreases as a function of MUs • Planning criteria: MU < 400 for 1/2 arcs
G(3,3) vs. accelerator • Differences between accelerators
Test plans used for QA • 6 of the test plans are use for QA 4 times a year each acc. • Plans with high G(3,3) are very stable (within 2-4%) Low/moderate modulation High modulation
Test plans used for QA • Some accelerators are more stable than others • Acc1 performs bad in autumn 2011 – no problems with mashine QC
Acc QC vs. Patient spec QC • Problems with acc QC on acc 5 (spring 2011) • Not seen for patient specific QC Low dose rate DRMLC test
Real patient plans • Reproducibility for each acc • Difference between acc – not seen with acc QC acc3
True beam • 5 patients treated at Clinac and True beam • G(3,3) does not depend on Clinac/True beam? • MeanG(Clinac)=98.4% • MeanG(TrueBeam)=99.0%
Portal dosimetry • Use EPID/MVD for patient specific QC • Fast measurement • Ideal for routine measurements
Delta4 vs. PDI • Perform Delta4 and PDI measurement consecutively at same accelerator • Preliminary results, Oct-Dec 2011: • 68 plans (1,2, ..6 arcs) • 127 single arcs • Single arcs • G(3,3)D4: • 1.7% higher than G(3,3)PDI • Plans • G(3,3)D4: • 1.0% higher than G(3,3)PDI • Pass criteria: • G(3,3)D4: 95% G(3,3)PDI: 94%
Work in Progress • Measurement of D4 and PDI for same plan at different accelerators • Analysis of data (approx 100 plans and 10 new plans pr week) • Workflow today: • Daily PDI; used for accept/reject • Weekly D4; used for check • Future: • Only PDI • New/additional machine QC program
Machine QC program • MV imager: • Test of ”clinical” dose rates • Test of reverse gantry direction • Test of gantry position • Delta4 • Still of measurement of 6 test plans 4xyear each accelerator