Download
1 / 14
140 likes | 297 Views
Medicare Modernization Act, Part D Prescription Drug Benefit. Presentation for County Program Administrators September 1, 2005. Timeline: When It All Happens. Timeline: When It All Happens. II. Impacts. On Client On County Clinicians On County Psychiatrists On County Budgets.

E N D
Medicare Modernization Act, Part DPrescription Drug Benefit Presentation for County Program Administrators September 1, 2005
II. Impacts • On Client • On County Clinicians • On County Psychiatrists • On County Budgets
Client Impacts • Client Awareness. Many of county mental health clients are isolated and do not have the benefit of family members to help them understand and navigate this process. • Coverage of PDP and/or MA-PD plans. • Formularies. CMS guidance indicates that PDPs and MA/PDs must cover “all or substantially all” medications in six pharmaceutical classes. • Step Therapy. PDPs and/or MA-PDs may require the use of step therapy prior to authorizing the payment of other medications. • Pharmacies May Not Contract with All PDPs or MA/PDs.
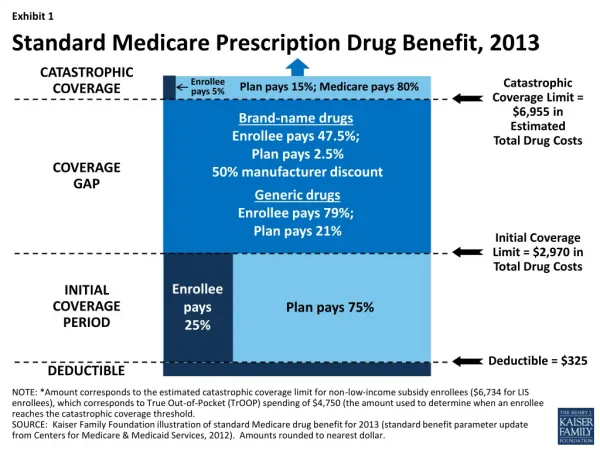
Client Impacts • Client Co-pays and Deductibles. • Extra Help Low Income Subsidy May Not Cover All the Costs. • For Medi-Medi clients, the transition period is insufficient. • Co-payments create an undue hardship • Cost control mechanisms may deny access to current medications (e.g. step therapy) • “Bait and switch” - plans offer generous, inclusive coverage initially and reduce access through subsequent plan amendments. • Coverage that Follows Client with Transitions to Other Levels of Care. • Transitional Levels of Care. There may be unintended consequences for transfers to other levels of care such as PHFs, IMDs, Jail, Juvenile Hall, etc.
Impact on Clinician Increased case management. • Educating clients • Cross-referencing plan coverage with psychotropic medication needs/prescriptions. • If client is not full benefit dual eligible, but is Medicare eligible, the clinician will need to help these individuals complete the “Extra Help” Low Income Subsidy. • Continuity of Care. Ensuring plan coverage takes place during transitions to other levels of care.
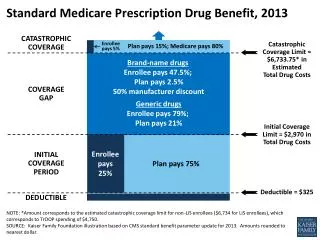
Impact on County Psychiatrists Formularies: Tier 1 is lowest cost sharing • Subsequent tiers have higher cost sharing in ascending order • CMS will review to identify drug categories that may discourage enrollment of certain people with Medicare by placing drugs in non-preferred tiers. • Plan must have exceptions procedures for tiered formularies. Psychiatrists will need to know what the exceptions procedures are. And, each plan may have different exceptions procedures.
Impact on County Psychiatrists • TAR Process.Knowledge and understanding of TAR process and which drugs will fall under the TAR. • Medication Coverage • Six classes (including antidepressants and antipsychotics). CMS guidance indicates PDPs and MA-PDs are required to cover “all or substantially all” medications. • Other health conditions may actually define consumer choice of PDPs or MA-PDs. • Knowledge of plan benefits and drug coverage.
Impact on County Mental Health • Increase in staff time for case management, both at the front end (enrollment) and through the Appeals Process. • Increase in staff time for administrative functions and problem resolution, including fiscal administration, navigating CMS system, and complaint/resolution process. • Increase in ER visits due to loss of eligibility and/or difficulty in navigating. • Depending upon county decisions, resources, and feasibility, counties could potentially be in the position of having to pick up a share or shares of cost.
III. Coordination with Inter-county agencies • County Welfare • “Extra Help” Low Income Subsidy. What directives do county welfare agencies want county mental health to follow in terms of enrolling clients in the LIS?
III. Coordination with Inter-county agencies • County Health Care • Who should be the “lead” in ensuring the client’s PDP/MA-PD plan covers all health medication needs and all mental health needs? • What kind of protocol makes sense? • What happens when a PCP changes a client’s health care medication and realizes that the medication is not covered under the client’s current PDP or MA-PD and advocates a change in plan for client? How will county mental health know about this change and how will it impact psychotropic script?
County Inter-agency • County Pharmacies • What role will county pharmacies play?