Download
1 / 1
10 likes | 191 Views
Primary Carcinosarcoma of the Liver: Radiologic and Pathologic Correlation 1 Midhir J. Patel, M.D., 2 Thora S. Steffensen, M.D., 1 Joseph R. Grajo, M.D. 1 University of South Florida, Department of Radiology, Tampa, FL 2 Tampa General Hospital, Department of Pathology, Tampa, FL. ABSTRACT.

E N D
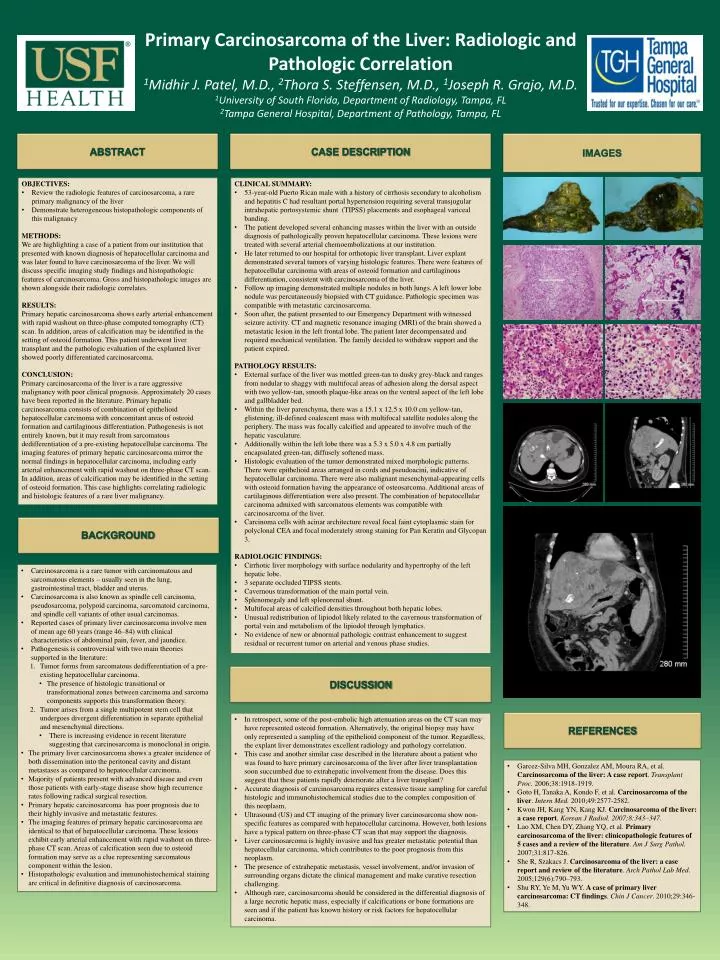
Primary Carcinosarcoma of the Liver: Radiologic and Pathologic Correlation1Midhir J. Patel, M.D., 2Thora S. Steffensen, M.D., 1Joseph R. Grajo, M.D.1University of South Florida, Department of Radiology, Tampa, FL2Tampa General Hospital, Department of Pathology, Tampa, FL ABSTRACT CASE DESCRIPTION IMAGES • OBJECTIVES: • Review the radiologic features of carcinosarcoma, a rare primary malignancy of the liver • Demonstrate heterogeneous histopathologic components of this malignancy • METHODS:We are highlighting a case of a patient from our institution that presented with known diagnosis of hepatocellular carcinoma and was later found to have carcinosarcoma of the liver. We will discuss specific imaging study findings and histopathologic features of carcinosarcoma. Gross and histopathologic images are shown alongside their radiologic correlates. • RESULTS:Primary hepatic carcinosarcoma shows early arterial enhancement with rapid washout on three-phase computed tomography (CT) scan. In addition, areas of calcification may be identified in the setting of osteoid formation. This patient underwent liver transplant and the pathologic evaluation of the explanted liver showed poorly differentiated carcinosarcoma. • CONCLUSION: Primary carcinosarcoma of the liver is a rare aggressive malignancy with poor clinical prognosis. Approximately 20 cases have been reported in the literature. Primary hepatic carcinosarcoma consists of combination of epithelioid hepatocellular carcinoma with concomitant areas of osteoid formation and cartilaginous differentiation. Pathogenesis is not entirely known, but it may result from sarcomatous dedifferentiation of a pre-existing hepatocellular carcinoma. The imaging features of primary hepatic carcinosarcoma mirror the normal findings in hepatocellular carcinoma, including early arterial enhancement with rapid washout on three-phase CT scan. In addition, areas of calcification may be identified in the setting of osteoid formation. This case highlights correlating radiologic and histologic features of a rare liver malignancy. • CLINICAL SUMMARY: • 53-year-old Puerto Rican male with a history of cirrhosis secondary to alcoholism and hepatitis C had resultant portal hypertension requiring several transjugular intrahepatic portosystemic shunt (TIPSS) placements and esophageal variceal banding. • The patient developed several enhancing masses within the liver with an outside diagnosis of pathologically proven hepatocellular carcinoma. These lesions were treated with several arterial chemoembolizations at our institution. • He later returned to our hospital for orthotopic liver transplant. Liver explant demonstrated several tumors of varying histologic features. There were features of hepatocellular carcinoma with areas of osteoid formation and cartilaginous differentiation, consistent with carcinosarcoma of the liver. • Follow up imaging demonstrated multiple nodules in both lungs. A left lower lobe nodule was percutaneously biopsied with CT guidance. Pathologic specimen was compatible with metastatic carcinosarcoma. • Soon after, the patient presented to our Emergency Department with witnessed seizure activity. CT and magnetic resonance imaging (MRI) of the brain showed a metastatic lesion in the left frontal lobe. The patient later decompensated and required mechanical ventilation. The family decided to withdraw support and the patient expired. • PATHOLOGY RESULTS: • External surface of the liver was mottled green-tan to dusky grey-black and ranges from nodular to shaggy with multifocal areas of adhesion along the dorsal aspect with two yellow-tan, smooth plaque-like areas on the ventral aspect of the left lobe and gallbladder bed. • Within the liver parenchyma, there was a 15.1 x 12.5 x 10.0 cm yellow-tan, glistening, ill-defined coalescent mass with multifocal satellite nodules along the periphery. The mass was focally calcified and appeared to involve much of the hepatic vasculature. • Additionally within the left lobe there was a 5.3 x 5.0 x 4.8 cm partially encapsulated green-tan, diffusely softened mass. • Histologic evaluation of the tumor demonstrated mixed morphologic patterns. There were epithelioid areas arranged in cords and pseudoacini, indicative of hepatocellular carcinoma. There were also malignant mesenchymal-appearing cells with osteoid formation having the appearance of osteosarcoma. Additional areas of cartilaginous differentiation were also present. The combination of hepatocellular carcinoma admixed with sarcomatous elements was compatible with carcinosarcoma of the liver. • Carcinoma cells with acinar architecture reveal focal faint cytoplasmic stain for polyclonal CEA and focal moderately strong staining for Pan Keratin and Glycopan 3. • RADIOLOGIC FINDINGS: • Cirrhotic liver morphology with surface nodularity and hypertrophy of the left hepatic lobe. • 3 separate occluded TIPSS stents. • Cavernous transformation of the main portal vein. • Splenomegaly and left splenorenal shunt. • Multifocal areas of calcified densities throughout both hepatic lobes. • Unusual redistribution of lipiodol likely related to the cavernous transformation of portal vein and metabolism of the lipiodol through lymphatics. • No evidence of new or abnormal pathologic contrast enhancement to suggest residual or recurrent tumor on arterial and venous phase studies. BACKGROUND • Carcinosarcoma is a rare tumor with carcinomatous and sarcomatous elements – usually seen in the lung, gastrointestinal tract, bladder and uterus. • Carcinosarcoma is also known as spindle cell carcinoma, pseudosarcoma, polypoid carcinoma, sarcomatoid carcinoma, and spindle cell variants of other usual carcinomas. • Reported cases of primary liver carcinosarcoma involve men of mean age 60 years (range 46–84) with clinical characteristics of abdominal pain, fever, and jaundice. • Pathogenesis is controversial with two main theories supported in the literature: • Tumor forms from sarcomatous dedifferentiation of a pre-existing hepatocellular carcinoma. • The presence of histologic transitional or transformational zones between carcinoma and sarcoma components supports this transformation theory. • Tumor arises from a single multipotent stem cell that undergoes divergent differentiation in separate epithelial and mesenchymal directions. • There is increasing evidence in recent literature suggesting that carcinosarcoma is monoclonal in origin. • The primary liver carcinosarcoma shows a greater incidence of both dissemination into the peritoneal cavity and distant metastases as compared to hepatocellular carcinoma. • Majority of patients present with advanced disease and even those patients with early-stage disease show high recurrence rates following radical surgical resection. • Primary hepatic carcinosarcoma has poor prognosis due to their highly invasive and metastatic features. • The imaging features of primary hepatic carcinosarcoma are identical to that of hepatocellular carcinoma. These lesions exhibit early arterial enhancement with rapid washout on three-phase CT scan. Areas of calcification seen due to osteoid formation may serve as a clue representing sarcomatous component within the lesion. • Histopathologic evaluation and immunohistochemical staining are critical in definitive diagnosis of carcinosarcoma. DISCUSSION • In retrospect, some of the post-embolic high attenuation areas on the CT scan may have represented osteoid formation. Alternatively, the original biopsy may have only represented a sampling of the epithelioid component of the tumor. Regardless, the explant liver demonstrates excellent radiology and pathology correlation. • This case and another similar case described in the literature about a patient who was found to have primary carcinosarcoma of the liver after liver transplantation soon succumbed due to extrahepatic involvement from the disease. Does this suggest that these patients rapidly deteriorate after a liver transplant? • Accurate diagnosis of carcinosarcoma requires extensive tissue samplingfor careful histologic and immunohistochemical studies due to the complex composition of this neoplasm. • Ultrasound (US) and CT imaging of the primary liver carcinosarcoma show non-specific features as compared with hepatocellular carcinoma. However, both lesions have a typical pattern on three-phase CT scan that may support the diagnosis. • Liver carcinosarcoma is highly invasive and has greater metastatic potential than hepatocellular carcinoma, which contributes to the poor prognosis from this neoplasm. • The presence of extrahepatic metastasis, vessel involvement, and/or invasion of surrounding organs dictate the clinical management and make curative resection challenging. • Although rare, carcinosarcoma should be considered in the differential diagnosis of a large necrotic hepatic mass, especially if calcifications or bone formations are seen and if the patient has known history or risk factors for hepatocellular carcinoma. REFERENCES • Garcez-Silva MH, Gonzalez AM, Moura RA, et al. Carcinosarcoma of the liver: A case report. Transplant Proc. 2006;38:1918-1919. • Goto H, Tanaka A, Kondo F, et al. Carcinosarcoma of the liver. Intern Med. 2010;49:2577-2582. • Kwon JH, Kang YN, Kang KJ. Carcinosarcoma of the liver: a case report. Korean J Radiol. 2007;8:343–347. • Lao XM, Chen DY, Zhang YQ, et al. Primary carcinosarcoma of the liver: clinicopathologic features of 5 cases and a review of the literature. Am J SurgPathol. 2007;31:817-826. • She R, Szakacs J. Carcinosarcoma of the liver: a case report and review of the literature. Arch Pathol Lab Med. 2005;129(6):790–793. • Shu RY, Ye M, Yu WY. A case of primary liver carcinosarcoma: CT findings. Chin J Cancer. 2010;29:346-348.