Download
1 / 36
410 likes | 721 Views
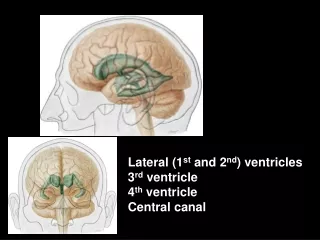
Ventricles Of Brain. Lateral Ventricle. lateral ventricles are the largest of the ventricles. They are irregular in shape. Each consists of a central part, with anterior, posterior and inferior horns. Anterior Horn of Lateral Ventricle.

E N D
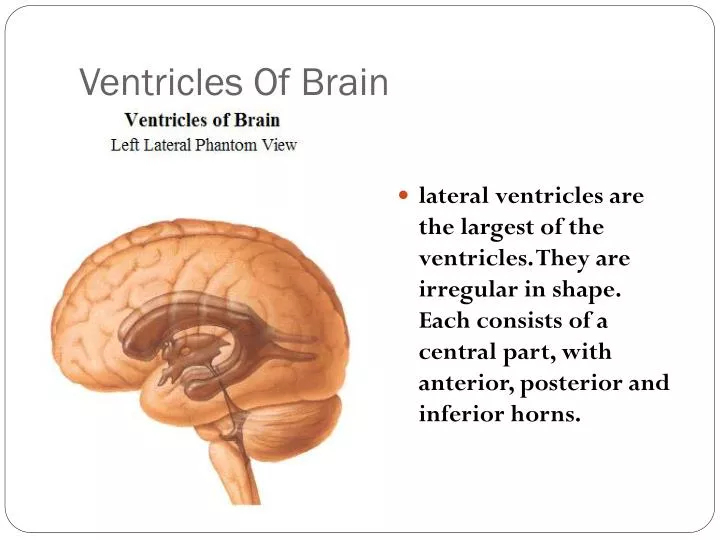
Ventricles Of Brain Lateral Ventricle lateral ventricles are the largest of the ventricles. They are irregular in shape. Each consists of a central part, with anterior, posterior and inferior horns.
Anterior Horn of Lateral Ventricle Anterior Horn is anterior to the interventricular foramen. Roof and anterior border are formed by the corpus callosum, Medial is Formed by the wall by the septum pellucidum. The floor is formed by the head of the caudate nucleus Anterior Horn
Body of lateral Ventricle • Extends from the splenium of the corpus callosum. • Medial Wall is Formed by the posterior part of the septum pellucidum. • Floor Is formed by the parts of the caudate nucleus, thalamus, choroid plexus and fornix.
Inferior Horn of Lateral ventricle • It traverses the temporal lobe. Its roof is formed by the white substance of the cerebral hemisphere. Along the medial border is the stria terminalis and the tail of the caudate nucleus. The amygdaloid nucleus bulges into the terminal part of the inferior horn. • The floor and the medial wall are formed by the fimbria, the hippocampus and the collateral eminence.
cerebrospinal fluid circulation • clear & colorless water-like fluid • formed by choroid plexus • mainly in lateral ventricles (& to lesser degree in 3rd & 4th ventricles) • formation of CSF complex • includes both passive filtration & active secretary mechanisms
CSF circulation • CSF produced in lateral ventricles • enters third ventricle through interventricular foramen • flows through cerebral aqueduct • into fourth ventricle • from fourth ventricle it reaches the subarachnoid space
CSF circulation • CSF enters subarachnoid space via three openings: • median aperture (posterior medullary velum) • two lateral apertures (lateral recesses of fourth ventricle)
CSF circulation • collections of microscopic arachnoid villi form macroscopic elevations (arachnoid granulations) that protrude into the lateral expansions of the superior sagittal sinus through openings in the dura • flow of CSF is fairly rapid
CSF circulation • total volume of CSF in the ventricular system & subarachnoid space is only about 125 ml • but it is estimated that about four times that amount (~500 ml) is formed during a 24 hr period • a small amount of CSF seeps down around the spinal cord
Case presentation • CC - A 9 month old infant is brought to his family physician because his parents are worried that the child’s head appears too large. • HPI- The mother had an apparently uneventful pregnancy and delivery. At birth the child’s body weight and head circumference were at 65th percentile (Normal)
Clinical Case cont.. • PE- Lethargic and irritable; anterior fontanellae bulging; when pressed slightly it immediately pops back; head circumference enlarged. • Lab-RPR( Rapid plasma reagin) in mother –ve (For syphilis).
Case Presentation • 29 year old woman is 32 weeks pregnant • She has complained of intermittent headache and • nausea for the last 16 weeks • Previous ER examinations have been normal • She collapses outside ER after 3rd visit and is • brought in comatose with extensor posturing and an dilated left pupil
HYDROCEPHALUS • DEFINITION: DIVERSE GROUP OF CONDITIONS WHICH RESULT FROM IMPAIRED CIRCULATION AND RESORPTION OF CSF.
CSF FORMATION • CSF IS FORMED BY THE CHOROID PLEXUS. • NORMAL CSF PRODUCTION: 20 ml/h.
TYPES OF HYDROCEPHALUS • OBSTRUCTIVE OR NON-COMMUNICATING (OBSTRUCTION WITHIN THE VENTRICULAR SYSTEM) • NON OBSTRUCTIVE OR COMMUNICATING (MALFUNCTION OF ARACHNOID VILLI)
CAUSES OF HYDROCEPHALUS • LESIONS OR MALFORMATIONS OF THE POSTERIOR FOSSA • CHIARI MALFORMATION • DANDY- WALKER SYNDROME • TUMORS • IVH • MENINGITIS: PNEUMOCOCCAL, TB • INTRAUTERINE INFECTIONS
PATHOLOGY • AQUEDUCTAL STENOSIS: • ABNORMALLY NARROW AQUEDUCTUS OF SYLVIUS. • AQUEDUCTAL GLIOSIS: • BRISK GLIAL RESPONSE OF EPENDIMAL LINING
CHIARI MALFORMATION • TYPE I: • DISPLACEMENT OF CEREBELLAR TONSILS INTO THE CERVICAL CANAL. • GIVES SYMPTOMS IN ADOLESCENCE OR ADULT LIFE. (HEADACHE, NECK PAIN) • NO HYDROCEPHALUS.
CHIARI MALFORMATION • TYPE II : • PROGRESSIVE HYDROCEPHALUS AND MYELOMENINGOCELE. • ELONGATION OF THE 4TH VENTRICLE. • DISPLACEMENT OF INFERIOR VERMIS, PONS, AND MEDULLA INTO CERVICAL CANAL
DANDY-WALKER SYNDROME • CYSTIC EXPANSION OF THE 4TH VENTRICLE IN THE POSTERIOR FOSSA. • DEVELOPMENTAL FAILURE OF ROOF OF 4TH VENTRICLE DURING EMBRYOGENESIS. • 90 % HAVE HYDROCEPHALUS • PROMINENT OCCIPUT
IVH • DEFINITION: • BLEEDING IN SUBEPENDIMAL GERMINAL MATRIX WITH/WITHOUT EXTENSION INTO VENTRICLES AND BRAIN PARENCHYMA • INCIDENCE: • IN PREMATURES 25 - 40 %
CLINICAL MANIFESTATIONS • SYMPTOMS: • IRRITABILITY • POOR FEED • LETHARGY • VOMITING • IN OLDER PATIENTS: • HEADACHE • CHANGES IN PERSONALITY • ACADEMIC DETERIORATION
CLINICAL MANIFESTATIONS • SIGNS: • ANTERIOR FONTANEL WIDE OPEN AND BULGING, INCREASED HEAD CIRC. • DILATED SCALP VEINS • SETTING SUN SIGN • BRISK TENDON REFLEXES, SPASTICITY • CLONUS, BABINSKY • MACEWEN SIGN “CRACKED POT” • PROMINENT OCCIPUT (DANDY-WALKER)
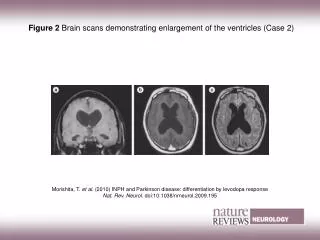
IMAGING STUDIES • X-RAY PLAIN FILMS: • SEPARATION OF SUTURES • EROSION OF POSTERIOR CLINOIDS • INCREASED CONVOLUTIONAL MARKINGS (BEATEN SILVER APPEAREANCE) • ULTRASOUND • CT SCAN • MRI