Download
1 / 75
750 likes | 978 Views
Psychological features of patients with therapeutic, surgical diseases. Psychological features of pregnant women and during birth giving. Features of psychology of sick children and old people. Functional somatic syndromes. Gastroenterology Irritable Bowel Syndrome Functional dyspepsia

E N D
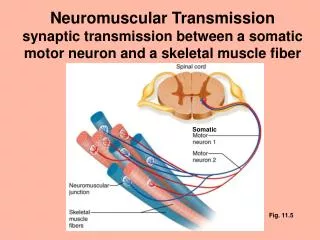
Psychological features of patients with therapeutic, surgical diseases. Psychological features of pregnant women and during birth giving. Features of psychology of sick children and old people.
Functional somatic syndromes Gastroenterology Irritable Bowel Syndrome Functional dyspepsia Cardiology Atypical chest pain Neurology Common Headache Chronic fatigue syndrome Rheumatology Fibromyalgia Complex regional pain syndromes Gynaecology Chronic pelvic pain Orthopaedics Chronic back pain
Suicide is… • 1. A form of behavior designed to deal with and solve a problem. • 2. A goal-oriented coping method. • 3. A way to take control. • 4. The ultimate revenge.
Why do People Commit Suicide? • I. PRIMARY REASONS • A. Hopelessness • B. Helplessness • II. PRE-SUICIDAL SITUATIONS • A. Sudden loss • B. Social isolation • C. Deep loneliness • D. Illness and pain • E. Changes in life style • F. Burden to others • G. Unfulfilled, unrealistic expectations
Some Common Characteristics of Suicidal People • A. Feelings of helplessness-sees the situation as intolerable and feels helpless to change it. • B. Feeling of hopelessness-sees the situation as having no solution therefore is unable to change it. • C. The individual experiences ambivalence-feels like dying but likes living at the same time. Ambivalence is the key in the intervention process. You must offer hope and strength to the side that wants to live, but also hear and understand the part seeking relief in the form of death. NEVER deny or ignore the side that wants to die. This will make the individual defensive and he/she will withdraw. • D. Suicide is rarely a spontaneous activity. It is usually a long drawn out process of depression and loss of ability to cope with stress, disappointment, etc.
Some Verbal and Behavioral Clues to Suicide Risk • REMEMBER: Any one clue does not equate suicide BUT a cluster of clues definitely warrants caution and intervention. Suicidal individuals give clues of their intent. These are verbal, blatant or coded, and behavioral messages we can listen for or be aware of.
VERBAL: • A. I'm going to kill myself. • B. My family would be better off without me. • C. I can't go on any longer. • D. I'm going on a trip/going to leave. • E. Please tell my family good-bye. • F. I wish I'd never been born. • G. You're going to be sorry when I'm gone. • H. I want to go to sleep and never wake up.
BEHAVIORAL: • A. Some abrupt behavior change in appearance, socialization, use/non-use of money, lessening of caution in dangerous situations. • B. A previous suicide attempt. • C. Giving away prized possessions • D. Putting business affairs in order. • E. Quick, unexpected recovery from deep depression. • F. A suicide note (some are written way before the attempt), death-related poems/stories/essays/journal entries.
Suicide Clues SITUATION REFERENCES • 1. I can't put my family through all the suffering and expense of these last few months. • 2. The doctor says there is no treatment for it. • 3. I don't know how I got into this mess, there's no way out. • 4. I've tried every drug program available, I've really tried, there's nowhere else to turn. • 5. I never thought I'd get caught. I can't face anyone after this. • 6. Nothing is going to make it any better. • 7. How can I be sure that my cats will be taken care of when I'm not there to do it? • 8. How does one leave their body to a medical school? • 9. Take care of my children. • 10. I've really tried but nothing works for me, nothing makes it right.
Suicide CluesSITUATION REFERENCES • 11. I just can't do the things I use to be able to do. • 12. I'd like to crawl into a hole and never come out. • 13. Sometimes I think I'd be better off dead. • 14. I just want out of the whole mess. • 15. That's one problem I'll never have to worry about again. • 16. I want out. • 17. I'm tired of trying. • 18. I have nothing to live for. • 19. The doctor says it's just a matter of time anyway. • 20. Everyone I ever loved is gone. • 21. I want you to tell my family good-bye for me.
RELATIONSHIP REFERENCES • 1. He/she will be better off without me. • 2. Nobody cares. • 3. He/she will be sorry when they find me. • 4. He/she will be sorry when they find out what I did. • 5. I can't wait to see his/her face when they find me dead. • 6. My mother is so angry with me because I won't have anything to do with her now. She thinks she has done something wrong but it just makes it easier this way. • 7. He deserves what I'm going to do to him. • 8. I've never been good enough for him it'll be better this way. • 9. Everything will be all right when my husband finds me. • 10. I'm going to make him suffer like I have. • 11. My children don't need me anymore-they'll be O.K.
TIME REFERENCES • 1. It won't matter after today. • 2. That doesn't matter now. • 3. I just can't go on like this anymore. • 4. I just called to say goodbye. • 5. You're the last person that will hear from me. • 6. That is one problem I am taking care of right now. • 7. I just want to sleep forever. • 8. I won't be around much longer anyway. • 9. I'm leaving. • 10. I've decided now…(pause)…it's time to do it.
TIME REFERENCES • 11. I can't take this any longer. • 12. Tomorrow…there won't be a tomorrow. • 13. That was a problem, a big problem, but it can't bother me now. • 14. I talked to all my family last night so everything is taken care of. • 15. About three months ago I went through a rough time and took an overdose, but I couldn't even pull that off. • 16. You can't help me now, nobody can. • 17. My sister killed herself a year ago today. • 18. I won't have any problems tomorrow. • 19. I don't have to worry about that anymore. • 20. You won't be hearing form me again. • 21. I can't live this way another day.
Myths about suicide • Suicide happens without warning. • Suicide people wish to die. • Once someone becomes suicidal, the person is always suicidal. • Once a persons depression has lifted, the danger of suicide is over. • Suicide is inherited and runs in families. • Suicidal people are mentally ill. • If someone is despondent, mentioning suicide will give the person suicide ideas.
Myths versus Facts • MYTH: People who talk about suicide don't complete suicide. • FACT: Many people who die by suicide have given definite warnings to family and friends of their intentions. Always take any comment about suicide seriously.
Myths versus Facts • MYTH: Suicide happens without warning. • FACT: Most suicidal people give clues and signs regarding their suicidal intentions.
Myths versus Facts • MYTH: Suicidal people are fully intent on dying. • FACT: Most suicidal people are undecided about living or dying, which is called “suicidal ambivalence.” A part of them wants to live; however, death seems like the only way out of their pain and suffering. They may allow themselves to "gamble with death," leaving it up to others to save them.
Myths versus Facts • MYTH: Men are more likely to be suicidal. • FACT: Men are four times more likely to kill themselves than women. Women attempt suicide three times more often than men do.
Myths versus Facts • MYTH: Asking a depressed person about suicide will push him/her to complete suicide. • FACT: Studies have shown that patients with depression have these ideas and talking about them does not increase the risk of them taking their own life.
Myths versus Facts • MYTH: Improvement following a suicide attempt or crisis means that the risk is over. • FACT: Most suicides occur within days or weeks of "improvement," when the individual has the energy and motivation to actually follow through with his/her suicidal thoughts. The highest suicide rates are immediately after a hospitalization for a suicide attempt.
Myths versus Facts • MYTH: Once a person attempts suicide, the pain and shame they experience afterward will keep them from trying again. • FACT: The most common psychiatric illness that ends in suicide is Major Depression, a recurring illness. Every time a patient gets depressed, the risk of suicide returns.
Myths versus Facts • MYTH: Suicide occurs in great numbers around holidays in November and December. • FACT: Highest rates of suicide are in May or June, while the lowest rates are in December.
Risk Factors • Psychiatric disorders • Past suicide attempts • Symptom risk factors • Sociodemographic risk factors • Environmental risk factors
Risk Factors Psychiatric Disorders Most common psychiatric risk factors resulting in suicide: • Depression* • Major Depression • Bipolar Depression • Alcohol abuse and dependence • Drug abuse and dependence • Schizophrenia *Especially when combined with alcohol and drug abuse
Risk Factors Other psychiatric risk factors with potential to result in suicide (account for significantly fewer suicides than Depression): • Post Traumatic Stress Disorder (PTSD) • Eating disorders • Borderline personality disorder • Antisocial personality disorder
Risk Factors Past suicide attempt (See diagram on right) • After a suicide attempt that is seen in the ER about 1% per year take their own life, up to approximately 10% within 10 years.* • More recent research followed attempters for 22 years and saw 7% die by suicide.** *Jenkins et al, BMJ, 2002 **Carter et al, BJP, 2007
Risk Factors Symptom Risk Factors During Depressive Episode: • Desperation • Hopelessness • Anxiety/psychic anxiety/panic attacks • Aggressive or impulsive personality • Has made preparations for a potentially serious suicide attempt* or has rehearsed a plan during a previous episode • Recent hospitalization for depression • Psychotic symptoms (especially in hospitalized depression) *Coryell W, Young et al, J Clin Psych, 2005
Risk Factors • Major physical illness, especially recent • Chronic physical pain • History of childhood trauma or abuse, or of being bullied • Family history of death by suicide • Drinking/Drug use • Being a smoker
Risk Factors Sociodemographic Risk Factors • Male • Over age 65 • White • Separated, widowed or divorced • Living alone • Being unemployed or retired • Occupation: health-related occupations higher (dentists, doctors, nurses, social workers) • especially high in women physicians
Risk Factors Environmental Risk Factors • Easy access to lethal means • Local clusters of suicide that have a "contagious influence"
Orthodox psychiatric view • The orthodox psychiatric view is that suicide is primarily the result of psychiatric disorder and is therefore predictable and preventable
Major depressive disorder and bipolar disorder are associated with at least 60% of suicides. • The lifetime risk of suicide of people with major depression is 3.4%, this is much lower than the commonly cited 15%, but still considerably higher than that of people free of psychiatric disorder. • Up to 83% of people who perform suicide have had contact with a physician in the year before their death
Research groups dedicated to the understanding and prevention of suicide conduct “psychological autopsies”, sifting through all the information available regarding the events of the individual’s life prior to suicide. They report evidence of diagnosable mental disorder in almost 90% of those who suicide and argue that the remaining 10% probably suffered a mental disorder which they were unable to detect
The prevention strategy • The prevention strategy drawn from these observations is for “improved screening of depressed patients by primary care physicians and better treatment of major depression ” • Suicide rates peak immediately after admission and discharge from psychiatric wards. The prevention strategy drawn from these observations is for “enhanced follow-up”
Schizophrenia is associated with a lifetime risk of completed suicide of 9 -13 and may be more lethal than depression. Other diagnoses, including anxiety, are also associated with greater risk
Risk factors • psychiatric disorder leading to hospitalization was the most prominent risk factor, but unemployment, low income, marital status, and family history of suicide additional important risk factors
Acute risk of suicide • Suicide risk may increase rapidly (acute suicide risk) as a result of sudden overpowering distress, in people both with and without mental disorder . • Wyder (2004) examined individuals who had survived a suicide attempt; 51% reported acting after thinking about their actions for 10 minutes or less. Of those who had been affected by alcohol, 93% had thought about their actions for 10 minutes or less. Impulsive acts make prevention problematic.
Acute risk of suicide • Acute suicide risk may occur in mental disorders, particularly psychotic depression, in which delusions of guilt and loss are prominent features. Mental disorders may be complicated by personality difficulties and the ready availability of alcohol. • Dumaiset al (2005) investigated cases in which suicide was completed during an episode of major depression. They found that impulsive-aggressive personality disorders and alcohol abuse/dependence were two important independent predictors of suicide in major depression.
Chronic risk of suicide • Chronic risk is a common feature of personality disorder, particularly b orderline personality disorder . The personality disorders differ from conditions such as major depressive disorder, which manifest episodes of difficulties. “Personality” refers to the characteristic (long-term) manner in which the individual responds to the environment.
Chronic risk of suicide • While personality disorder is a chronic condition, there may be superimposed periods of more acute distress and risk of suicide. Borderline personality disorder , characterized by a pervasive pattern of instability of interpersonal relationships and mood, and marked impulsivity, has a 10% lifetime risk of suicide. Impulsive suicide is usually triggered by adverse life events.
Illustration. ThichQuangDuc burned himself to death in Saigon (Vietnam) in 1963. He was protesting the way, in his view, the government was oppressing the Buddhist religion.
Illustration. Jo Shearer, a 56 year old accomplished journalist who suffered intractable pain. She advised colleagues of her intention and ended her life.
The sociological model • “Experience indicates that for effective suicide prevention, the appropriate treatment of people with mental disorders is just one of the main component s. Actually, biological and psychological characteristics, and factors pertaining to the cultural, social and physical environment, although more difficult to approach in quantitative ways, should receive much more attention…” • Bertolote et al, 2004
Durkheim’s classification of suicide. • Egoistic suicide occurs when an individual is inadequately integrated into society, and is lonely and socially isolated. Altruistic suicide occurs when the individual is too tightly integrated into society and places the needs of the society above his or her own; examples include the Kamikaze pilot or the suicide bomber. • Anomic suicide is the most common and occurs when anomie occurs. Anomie is the condition where social and/or moral norms are confused, unclear, or simply not present . Durkheim observed anomie and the loss of traditional values, as a result of industrialization. This is also evident in current society, in which we are increasingly separated and divided by computer technology, the internet, increasing bureaucracy, and specialization in the workplace. Durkheim rejected pathological mental states as a class of causes of suicide. At most he would concede that a pathological mental state may predispose an individual to commit suicide. The causes, he maintained, were social. In a reassessment of “Suicide”, Durkheim’s dismissal of mental illness as a key determinant of suicide has been described as “baseless”, but his conceptualization of anomic, ego istic and altruistic suicide has been accepted as providing “a means of comprehending recent trends in suicidal behavior” (Robertson, 2006).
The impact of social factors (in pa rticular, anomie) on suicide rates is currently well demonstrated in the North America n Indians, who have the highest suicide rate of all ethnic groups in the United States. This culture is under extreme pressure and family conflict, alcohol abuse and hopelessness are believed to be important factors leading to suicide. • The 2003 SARS epidemic in Hong Kong was associated with a marked increase in the suicide rate of the elderly, and biopsychosocial factors have been implicated. Psychosocial stresses have been associated with the suicidal behavior of adolescents in rural china.
The importance of social factors in suicide was recently highlighted in Australia. Page et al (2006) found that across the period 1979 -2003, socioeconomic status differentials in suicide persisted for both men and women. Low socioeconomic status was consistently associated with higher suicide rates, high socioeconomic status was consistently associated with lower rates and middle socioeconomic status was consistently associated with a suicide rate between these extremes.