Download
1 / 15
190 likes | 464 Views
The Health Care Delivery System Part One. Craig A. Pedersen, R.Ph., Ph.D. Department of Pharmaceutical and Administrative Sciences School of Pharmacy Ohio State University. Objectives for Parts 1 and 2.

E N D
The Health Care Delivery SystemPart One Craig A. Pedersen, R.Ph., Ph.D. Department of Pharmaceutical and Administrative Sciences School of Pharmacy Ohio State University
Objectives for Parts 1 and 2 • After viewing and listening to the lecture posted on Blackboard, the student will be able to: • Name the three cornerstones of a health care delivery system and discuss what has happened in the current market. • Explain at least two methods of measuring quality and access. • Assess how risk sharing affects providers in the student’s profession.
Objectives cont. • List at least six reasons for why the percentage of people covered by managed care plans has increased considerably in the last decade. • State her/his preference for managed care plan type and explain the choice. • Explain how managed care has changed the roles of health professionals.
Health Care Delivery SystemDesign Principles Price Access Quality
Health Care Delivery System Design Principles Emphasized in the Current Market Price Access Quality Health Plan Quality has been difficult to define and measure.
1. Taxation 2. Employer Payment 3. Individual Payment 4. Philanthropy Sources of Funds to Pay for Health Care
1. Price of Service (Unit price for each service rendered) 2. Quantity of Services (Number of Unit of service rendered) 3. Cost of Administration (Cost of collecting and paying for services) Three Components that Determinethe Cost of a Health Plan x + = Premium Price = Total Health Plan Cost ___________________________ Total Health Plan Enrollment Total Health Plan Cost
Relationship between Financingand Utilization in Health Care • If price per unit of service is negotiated, but the number of services is allowed to rise indiscriminately, the total price for health care may continue to increase. • Cost control in health care delivery is a balance between controlling the cost per unit of service and the controlling the total number of services that are provided and reimbursed.
Price • Focus originally was on physicians and hospitals • Focus expanded to include PT, OT, lab, pharmacy, etc. • Purchasing Power - required to obtain concessions - Market dominance?
Structure Process Outcome # of board certified specialists Time to obtain trauma care services Degree of satisfaction among enrollees Quality Donabedian A. Evaluating the quality of medical care. Milbank Mem Fund Q 1966;44:33-49.
Access • Proximity • Number of Providers • Type of Providers (general practice or specialty) • Number of Hospitals • Waiting times
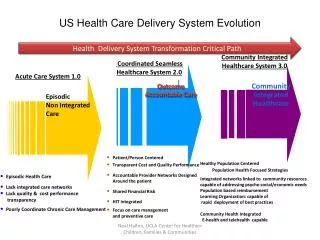
Dominant Methods of HealthCare Service Reimbursement: • Fee for Service: Payment for each and every service rendered by the professional or institution as defined by the professional or institution. Provider is at NO RISK. • Episode of Care: Payment for an entire episode of care based on an established measure of that episode (i.e. Diagnosis Related Groups or DRG’s). Provider is at PARTIAL RISK. Both in-patient and out-patient are now on DRGs. • Capitation: Partial capitation is payment in advance for pre-defined, predictable services on the basis of a specific per member per month amount. Complete capitation is payment for all services in advance on the basis of a specific per member per month amount. Provider is at PARTIAL to FULL RISK.
The Trend in Provider Payment is toward more RISK SHARING • Risk sharing is a concept that puts the provider of health care at some risk for the total annual cost of a health care plan. Episode of Care and Capitation reimbursement are most commonly used to share risk and, it is assumed, extend greater performance responsibility to the provider for the health care that is provided.
Why Managed Care? A brief history of how we got here • Reimbursement philosophy that rewarded service use and expansion regardless of capacity. • Proliferation of resources without any market oriented demands for efficiency. • Rising consumer expectations for cure. • Highest rewards given for new technology: - Expansion of Specialization - Focus on Acute rather than Preventive. • Services are defined by provider (or seller) rather than consumer (or market). • Increasing litigation & malpractice costs. • Aging society with greater health care needs. • High cost administrative and regulatory bureaucracy.