Download
1 / 23
230 likes | 368 Views
Cardiovascular System: The Heart. Chapter 18. Heart Anatomy w/Review. Size of a fist In the mediastinum Obliquely situated ___?_____ to the diaphragm ___?_____ to the vertebral column ___?_____ to the sternum Lungs are ___?_____ and slightly obscure it

E N D
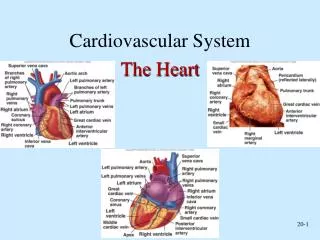
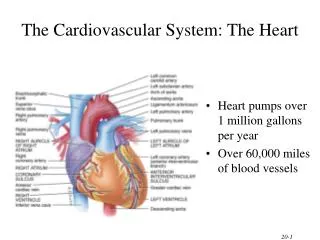
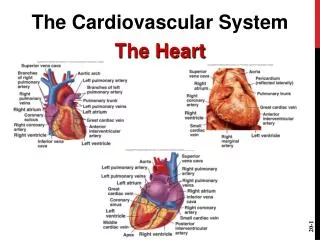
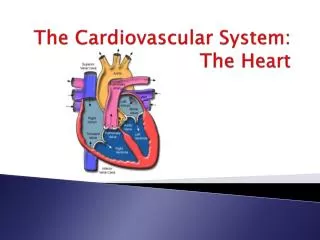
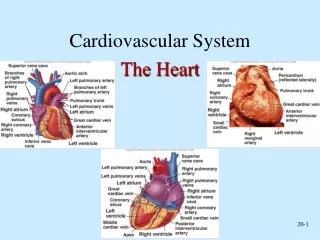
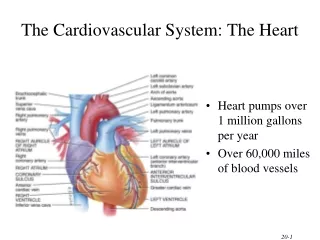
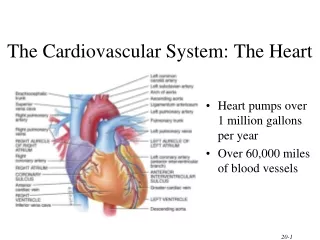
Cardiovascular System: The Heart Chapter 18
Heart Anatomy w/Review • Size of a fist • In the mediastinum • Obliquely situated • ___?_____ to the diaphragm • ___?_____ to the vertebral column • ___?_____ to the sternum • Lungs are ___?_____ and slightly obscure it • Base is right and posterior, apex is point
Pericardium • Serous membrane surrounding the heart • Protects, anchors, and prevents overfilling • Fibrous pericardium,collagen and elastic figure 8’s • Link all parts together while providing additional support • Limits AP spread • 2 layers • Parietallayer covers the _____?_____ • Visceral layer (epicardium) covers the _____?___ • Pericardial cavity between w/ serous fluid
Heart Wall • Epicardium (visceral pericardium) • Fatty layer • Myocardium • Cardiac muscle • Endocardium • Simple squamous epithelia • Continuous with blood vessels • Forms valves www.faculty.ccri.edu
Chambers of the Heart • 2 superior atria • Interatrial septum • Coronary sulcus • 2 inferior ventricles • Interventricular septum • Anterior and posterior ventricular sulcus • REMEMBER: directions for specimen/model NOT self http://www.nku.edu/~dempseyd/HEART_1.htm
Atria of the Heart • Receiving chambers • Auricles to increase volume • Pectinate muscles internal, anterior walls • Fossa ovalis: remnant of fetal opening • Right entry (O2 poor from systemic) • Superior and inferior venae cavae • Coronary sinus • Left entry (O2 rich from pulmonary) • Right and left pulmonary veins http://www.google.com/imgres?imgurl=http://www.washingtonhra.com/resources/Heart%2Banatomy.png&imgrefurl=http://www.washingtonhra.com/2.html&usg=__6-rsXPk2HfBZ4NNeV1B4Gs7DIgI=&h=500&w=342&sz=454&hl=en&start=0&zoom=1&tbnid=hUO3hlsVbY8FXM:&tbnh=143&tbnw=98&prev=/images%3Fq%3Datrium%2Banatomy%26um%3D1%26hl%3Den%26sa%3DN%26biw%3D834%26bih%3D667%26tbs%3Disch:1&um=1&itbs=1&iact=rc&dur=414&ei=K4pxTIzAFsP38AaI2o2ACw&oei=K4pxTIzAFsP38AaI2o2ACw&esq=1&page=1&ndsp=12&ved=1t:429,r:0,s:0&tx=48&ty=73
Ventricles of the Heart • Discharge chambers • Trabeculaecarneae, folds of muscle • Papillary muscles • Right (anterior) exit • Pulmonary trunk • Right and left pulmonary arteries • Left (posterior) exit • Aorta http://www.google.com/imgres?imgurl=http://www.washingtonhra.com/resources/Heart%2Banatomy.png&imgrefurl=http://www.washingtonhra.com/2.html&usg=__6-rsXPk2HfBZ4NNeV1B4Gs7DIgI=&h=500&w=342&sz=454&hl=en&start=0&zoom=1&tbnid=hUO3hlsVbY8FXM:&tbnh=143&tbnw=98&prev=/images%3Fq%3Datrium%2Banatomy%26um%3D1%26hl%3Den%26sa%3DN%26biw%3D834%26bih%3D667%26tbs%3Disch:1&um=1&itbs=1&iact=rc&dur=414&ei=K4pxTIzAFsP38AaI2o2ACw&oei=K4pxTIzAFsP38AaI2o2ACw&esq=1&page=1&ndsp=12&ved=1t:429,r:0,s:0&tx=48&ty=73
Heart Valves • Keep single directional blood flow • Open/close due to pressure not contraction • Atrioventricular valves (AV) • Right is tricuspid • Left is bicuspid or mitral • Anchored to papillary muscles by chordae tendineae‘heart strings’ • Semilunar valves (SL) • Aortic • Pulmonary
Valve Function • AV • Returning blood to atria exerts pressure = valves open to ventricle • Ventricles contract = increase pressure = valves close • Chordae tendineae and papillary muscles prevent inward flip • SL • Ventricles contract = increase pressure = valves open • Ventricles relax = blood flows back = close valves
Coronary Circulation • Arterial supply in coronary sulcus • Right coronary splits • Marginal: lateral right myocardium • Posterior interventricular: heart apex and posterior ventricular walls (join for right atria and ventricle) • Left coronary splits • Circumflex: left atria and posterior wall of left ventricle • Anterior interventricular: interventricular septum and anterior ventricle walls (join for right atria and ventricle) • Actually varies between individuals • Venous supplies join in coronary sinus • Great cardiac in anterior interventricular sulcus • Middle cardiac in posterior interventricular sulcus • Small cardiac w/marginal artery
Cardiac Muscle Anatomy • Intercalated discs • Gap junctions: passage/exchange of ions • Desmosomes: stabilize and maintain structure • Heart behaves as a single unit • Other characteristics (review) • Nuclei #? • Control? • Structure?
Cardiac Muscle Contraction • Neural stimulation not needed = autorhythmicity • Can influence pace • Whole organ (not just motor units) contracts • Signals carried through gap junctions • Longer absolute refractory period • Regulates contraction rate • Prevents sustained contraction (tetanus) • Lots of mitochondria • Greater dependence on O2 • Presence of fuel source more important than type
Autorhythmic Cells • Initiate action potentials in the heart • Due to pacemaker potential or unstable resting period • Basic steps of an AP (review) • Changes • Continuous depolarization to threshold (no flat line) • Ca2+channels open and Ca2+ rushes in • AP NOT triggered by Na+ • Found in specific locations • Sinoatrial and atrioventricular nodes • Right and left bundle branches • Ventricular walls (Pukinje fibers)
Beating to It’s Own Drum • Sinoatrial (SA) node or ‘pacemaker’ • Depolarization rate is fastest • Impulse ~75 times/min • Atrioventricular (AV) node delays impulse • Bundle of His electrically connects chambers • Bundle branches to apex • Pukinje fibers to contractile fibers in ventricles
Extrinsic Heart Control • Cardiac centers in medulla • Cardioacceleratroy center • Sympathetic NS • Pre- from T1-T5 up • Post- through cardiac plexus to SA and AV nodes & arteries • Cardioinhibitory center • Parasympathetic NS • Pre- from vagus to heart • Post- to SA and AV nodes
Electrocardiogram (ECG or EKG) • Records all electrical autorhythmic cell activity • Distinguishable waves • P wave: SA node depolarizes atria • Atria contracts • Drop from AV node delay • QRS complex: ventricle depolarization • Ventricle contracts • Masks atrial repolarization • T wave: ventricle repolarization
Heart Sounds • ‘Lub’ when AV valves close • Ventricular systole (contraction) begins • Bicuspid (mitral) before tricuspid • ‘Dup’ when SL valves close • Ventricular diastole (relaxation) begins • Aortic before pulmonary • Listen to 4 regions for differences
Cardiac Cycle • Ventricular filling • Relaxed chambers creates low pressure allows passive blood flow in • Atria contract, ‘topping off’ ventricles = end diastolic volume (EDV) • Ventricular systole (contraction) • Ventricles contract increasing pressure (isovolumetric contraction phase) • AV valves close and SL valves open • End systolic volume (ESV) remains • Early diastole • Ventricles relax decreasing pressure (isovolumetric relaxation phase) • SL valves close
Cardiac Output (CO) • Amount of blood pumped by each ventricle • CO (ml/min) = HR (beats/min) x SV (ml/beat) • Stroke volume (SV) is amount of blood per ventricular contraction • Variable and increases with demand • Max CO – rest CO = cardiac reserve • Athletes have higher
Regulating Stroke Volume • SV = EDV – ESV • EDV is amount of blood in ventricle during diastole • ESV is amount of blood in ventricle after systole • Affecting factors • EDV by preload: degree of cardiac stretch pre-contraction in ventricles • Slow HR increases volume of return • Exercise increases speed of return • ESV by contractility: contractile force of cardiac cells • SNS innervation, Ca2+ entry, and hormones increase • More blood leaves = decrease in ESV • Ca2+ blockers, increased extracellular K+ , and acidosis decrease • ESV by afterload: pressure needed to eject blood • High BP more difficult to eject blood = increased ESV
Regulating Heart Rate • ANS • SNS stimulates with stress, excitement, or exercise • PNS stimulates with ACh and opposes SNS • Majority of autonomic stimuli; slows heart rate • Chemical controls • Hormones: epinephrine, norepinephrine, and thyroxine increase • Ions • Other factors • Temperature • Age and exercise
Homeostatic Imbalances • Pericarditis: inflammation of pericardium roughens serous membrane • Cardiactamponade: heart is compressed by fluid in pericardial cavity • Angina pectoris: deficient blood flow to myocardium • Myocardial infarction: prolonged coronary blockage; heart attack • Incompetent valves: valves fail to close allowing blood backflow • Stenosis: valves are stiff or obscure opening; heart must work harder • Ischemia: depriving tissue of oxygen • Arrhythmia: uncoordinated atrial/ventricular contractions • Fibrillation: rapid, out of phase contraction • Heart block: AV node damage; ventricles contract on own • Heart murmurs: blood swooshing; valves fail to close • Tachycardia: abnormally fast HR; stress, drugs, or temp cause • Bradycardia: abnormally slow HR; drugs, endurance training, or PNS