Download
1 / 24
260 likes | 968 Views
Malaria …. … thy cunning seeds, Oh, million-murdering Death. - Ronald Ross. Malaria. From the Italian “mal aria” - Bad Air Also known as ague, marsh disease Descriptions of malaria go as far back as 3550 B.C. Caused by species of the genus Plasmodium . There are nine sub-genera.

E N D
Malaria… …thy cunning seeds, Oh, million-murdering Death. -Ronald Ross
Malaria • From the Italian “mal aria” - Bad Air • Also known as ague, marsh disease • Descriptions of malaria go as far back as 3550 B.C. • Caused by species of the genus Plasmodium. • There are nine sub-genera. • Three occur in mammals • Four occur in birds • Two occur in lizards
Taxonomy • Kingdom: Animalia • Phylum: Apicomplexa • Class: Coccidia • Order: Haemosporidia • Genus: Plasmodium • Species: vivax, falciparum, ovale & malariae
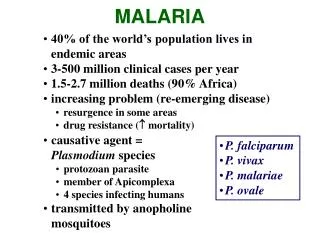
Parasitic Human Malarias • Of the nine sub-genera, there are four that are typically parasitic to humans • P. falciparum • P. vivax • P. malariae • P. ovale • Each is more closely related to other Plasmodium lineages than each other
Hosts of Plasmodium • Plasmodium requires two types of host • Vertebrate and Invertebrate • Definitive host is the invertebrate (Anopheles spp.) • Sexual reproduction occurs • Intermediate host is the vertebrate (Humans) • Asexual reproduction occurs
Reproduction and maturation in definitive host • Anopheles spp. ingest erythrocytes containing Plasmodium gametocytes • If an unsuitable species of mosquito ingests Plasmodium gametocytes, they are digested • Macrogametocytes and Microgametocytes are released from erythrocytes • Macrogametocyte matures into macrogamete (Nucleus shift) • Microgametocyte matures into microgamete (exflagellation) • Microgametes fertilize macrogametes • Diploid zygote becomes a motile ookinete
Reproduction and maturation in definitive host, cont’d • The motile ookinete penetrates the stomach lining of the mosquito • Once there, the ookinete begins to form an oocyst • Sporoblasts begin to form within the oocyst • Sporoblasts divide repeatedly to form sporozoites • Sporozoites break out of the oocyst and migrate throughout the body of the mosquito • This entire process (from ookinete to sporozite) can take from 10-21 days • Some sporozoites end up in the salivary gland of Anopheles, where they are transmitted when the mosquito takes a blood meal
Reproduction and maturation in the intermediate host • Sporozoites injected by Anopheles migrate to liver from the bloodstream • Covered in a protein that aids in access to hepatocytes • Entry into hepatocytes is the beginning of the pre-erythrocytic cycle • Upon entry into hepatocytes, sporozoites become feeding trophozoites • Some sporozoites go dormant indefinitely (depending on Plasmodium spp) • After a week, trophozoites are mature • At this point, trophozoites undergo schizogony
Reproduction and maturation in the intermediate host, cont’d • Merozoites re-enter the blood from the liver and penetrate red blood cells • Upon entry, merozoites become trophozoites again • At this stage, trophozoites display distinctive “signet-ring” appearance, feed on hemoglobin • After maturing in the RBC, trophozoites again form a schizont, creating more merozoites • RBC ruptures, releasing merozoites, and parasite metabolic wastes, which causes many of the symptoms of malaria • One of these, hemozoin, a byproduct of parasitic consumption of hemoglobin, is toxic, and causes inhibition of macrophages • After a number of generations, some merozoites become macro and microgametocytes • Ingestion of gametes causes infection in Anopheles • If not ingested, gametes are phagocytized
P. falciparum • Is the most dangerous of the malaria parasites • Accounts for 50 % of all malaria cases • Causes malignant tertian malaria • Symptoms appear 9 to 14 days after initial infection • Parasitemia levels are extremely high • Up to 65% of erythrocytes infected • Schizonts grow in liver cells • Schizont ruptures in 5 1/2 days, releasing 30,000 merozoites • Schizonts are more asymmetrical than other Plasmodium spp. • Infected RBCs can attach to uninfected RBCs, forming rosettes • Rosettes can clog venules • Falciparum trophozoites secrete proteins that cause deformations of erythrocytes • Falciparum trophozoites extend pseudopodia, but are not as active as P.vivax trophozoites • Falciparum gametocytes are crescent shaped
P.vivax • Trophozoites of P.vivax are much more motile than other plasmodium spp. • This motility caused Italian researchers to nickname it “vivace”, Italian for “quick and lively” • P.vivax flourishes in temperate zones • Most cases of P.vivax malaria now occur in Asia • P.vivax is common in North Africa, but not in tropical Africa • Africans have a natural resistance to this form of malaria • Schizonts are formed in the liver parenchyma and release 10,000 merozoites upon maturation • Trophozoites cannot penetrate mature red cells • In addition, merozoites can only penetrate RBCs with mediated receptor sites • Receptor sites are genetically determined, conferring resistance • A defining characteristic of P.vivax is the development of hypnozoites • Hypnozoites cause relapse of malarial infection
P.vivax, cont’d • P.vivax gametocytes are rounded • It appears that P.vivax gametocytes do not require several generations to appear • Causes benign tertian malaria • Symptoms appear between 12 and 18 days after initial infection
P. Malariae • Causes quartan malaria • Causes paroxysms every 72 hours • Is cosmopolitan, but does not have continuous distribution • Is found in many regions of tropical Africa, Asia, South America, and even Europe • Is thought to be the only Plasmodium organism that lives in wild animals • Parasitemia levels are low • One parasite per 20,000 red cells • Symptoms appear between 18 and 40 days after initial infection
P. Ovale • Rarest of the four malaria parasites • Causes tertian malaria • Symptoms appear between 12 and 18 days after initial infection • Common to western coastal Africa, also found in India, the Philippines, New Guinea, and Vietnam • Difficult to diagnose due to its similarity to P.vivax • Gametocytes take longer to appear in blood than those of other species
Symptoms • Common symptoms • Fever • Chills • Headache • Sweats • Fatigue • Nausea and vomiting • P.falciparum • Causes Cerebral Malaria, which accounts for 10 % of hospital admitted malaria cases and 80% • Mild jaundince • Enlarged liver • Increased respiratory rate • Pulmonary edema • P.vivax • P.ovale • P.malariae
Pathogenesis • Clinical signs of malaria can be attributed to two factors • Host inflammatory response • Produces chills and fever • Correlated with maturation of merozoites, rupture of RBCs • Toxins released from burst RBCs can stimulate secretion of TNF by macrophages • TNF overproduction and toxicity can cause most or all of malaria symptoms • Anemia • Caused by destruction of RBCs
Diagnosis • Diagnosis of malaria can be difficult, because many symptoms are general • Demonstration of the parasites in peripheral blood is important to a diagnosis • Individuals with very low parasitemias can often be overlooked • Several effective methods for diagnosis have been developed • Fluorescent dye staining • DNA probe specific for P.falciparum • PCR diagnostics • ELISA detection of P.falciparum antigen
Treatment • Treatment of malaria focuses on eradication of the blood parasites • Several drugs can be administered, such as • Chloroquine • Quinine • Doxycycline • Malarone • Lariam • Fansidar • Treatment is dependent on several factors, including: • Type of malaria • Drug-resistance • Nearly all strains of P.falciparum are now chloroquine resistant, in addition to developing resistance to nearly all other currently available antimalarial drugs • P.vivax has also developed resistance to chloroquine and primaquine, though they are not as widespread as P.falciparum
Impact of malaria • According to the WHO - World Malaria Report 2005: • At the end of 2004, some 3.2 billion people lived in areas at risk of malaria transmission in 107 countries and territories. • Between 350 and 500 million clinical episodes of malaria occur every year. • At least one million deaths occur every year due to malaria. • About 60% of the cases of malaria worldwide and more than 80% of the malaria deaths worldwide occur in Africa south of the Sahara. • In 1995, 990,000 deaths reported in some African countries where malaria infection is high (2,700 deaths per day) • In 2000, 84% of the blood transfusion given in Kinshasa, Congo were for anemia caused by malaria