Download
1 / 26
301 likes | 2.06k Views
Marfan Syndrome. Stephanie van Colen, DO. Marfan Syndrome. Marfan syndrome is an inherited connective tissue disorder Autosomal dominant Results from molecular defects in the fibrillin gene , (FBN1) on chromosome 15 (q15-q21)

E N D
Marfan Syndrome Stephanie van Colen, DO
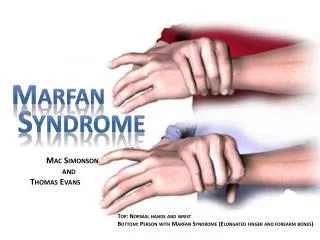
Marfan Syndrome • Marfan syndrome is an inherited connective tissue disorder • Autosomal dominant • Results from molecular defects in the fibrillin gene, (FBN1) on chromosome 15 (q15-q21) • Impaired structural integrity of the skeletal, ocular, and cardiovascular systems
Features • Tall stature • Mitral-valve prolapse • Aortic-root dilatation • Aortic dissection • Pectus deformities • Occular problems - ectopia lentis • Joint laxity • Spinal deformities
Pathophisiology • The affected gene encodes for the glycoprotein fibrillin: a major building block of microfibrils - structural components of the suspensory ligament of the lens - elastin in the aorta and other connective tissues
Pathophysiology • Abnormalities in the microfibrils - weaken the aortic wall • Progressive aortic dilatation and possible aortic dissection secondary to tension caused by left ventricular ejection • Deficient fibrillin - reduced structural integrity of the lens zonules, ligaments, lung airways, and spinal dura
In patients with Marfan’s, the media is affected and has decreased tensile strength
Physical Findings • The diagnosis of Marfan syndrome is mainly clinical • Skeletal findings • Taller/thinner stature • Limbs are disproportionately long compared with the trunk (dolichostenomelia) • Arachnodactyly
Physical Findings • Major criteria include the following: • Pectus excavatum (severe)/ pectus carinatum • Reduced upper-to-lower body segment ratio • Arms and legs may be unusually long in proportion to the torso • Positive wrist (Walker) and thumb (Steinberg) signs • Scoliosis greater than 20°: > 60% of patients • Reduced extension of the elbows (<170°) • Medial displacement of medial malleolus - pes planus • Protrusio acetabula of any degree
Positive thumb (Steinberg) sign Positive wrist (Walker) sign
Physical Findings • Minor criteria are as follows: • Pectus excavatum (moderate) • Scoliosis less than 20° • Thoracic lordosis • Joint hypermobility • Highly arched palate • Dental crowding • Typical facies (dolichocephaly, malar hypoplasia, enophthalmos, retrognathia, down-slanting palpebral fissures) • For the skeletal system to be involved, need 2 major criteria or 1 major criterion plus 2 minor criteria
Other systems • Ocular findings: • The major criterion is ectopia lentis; @ 50% • Multiple other ocular findings • Pulmonary findings: • Minor criteria include the following: • Spontaneous pneumothorax (about 5%) • Apical blebs • Dural findings: • 1 major criterion is defined: Dural ectasia (seen on CT / MRI) • Seen in 65-92%, usually in the lumbosacral spine • Dural ectasia: ballooning / widening of the dural sac +/- herniation of the nerve root sleeves out of the foramina • Less than 20% of patients have serious dural ectasia
Cardiovascular • Major criteria: • Aortic-root dilatation: ( 70-80%) • Aortic dissections involving the ascending aorta • Minor criteria: • Mitral valve prolapse (55-69%) • Dilatation of proximal main pulmonary artery without pulmonic stenosis or other cause • Calcification of mitral annulus (patients <40 y) • Dilatation of abdominal or descending thoracic aorta (patients <50 y) • For the CV system to be involved, need 1 minor criterion
Differential • Ehlers-Danlos Syndrome • Fragile X syndrome • Gigantism and acromegaly • Hyperpituitarism • Hyperthyroidism • Klinefelter syndrome
Echocardiography • Diagnosis and management of aortic-root dilatationThe upper limit of the normal aortic root size is 1.9 cm/m2 of body surface area • Assesses mitral-valve prolapse, LV size / function, LA size, and tricuspid valve function • TEE assesses the distal ascending and descending aorta and prosthetic valves • Doppler echocardiography - detecting and grading aortic and mitral regurgitation
CT and MRI • MRI for assessing chronic dissection of the aorta- any patient who has an aortic-root dimension >150% of the mean for their body surface area or - ratio of actual to predicted aortic-root dimension >1.5 • CT or MRI of the lumbosacral spine to evaluate for dural ectasia
Treatment • Cardiovascular surgery • CV surgery can substantially prolong survival Prophylactic / emergency CV surgery is needed for:- aortic and mitral regurgitation - aortic aneurysm- aortic dissection • In cases of acute proximal aortic dissection, emergency surgical replacement of the aortic root is performed
Treatment • The ascending aorta is usually replaced when the diameter exceeds 55-60 mm • Composite valve-graft replacement is performed - prosthetic valve sewn into a tube graft with reimplantation of the coronary ostia (modified Bentall procedure) • Low rates of morbidity and mortality
Treatment • Bentall procedure • Repair of Type A aortic dissection, aneurysm of the proximal ascending aorta, and aortoannular ectasia • Replacement of the root and proximal ascending aorta with a tube graft containing a prosthetic valve and reimplantation of the coronary arteries into the graft • Postoperative complications include: • leakage at the suture lines - pseudoaneurysm of the aortic or coronary anastomosis
Non-cardiac Treatment • Scoliosis surgery • Pectus repair • Repair of pectus excavatum to improve respiratory mechanics • Pectus carinatum repair - mainly for cosmetic reasons • Pneumothorax therapy • Ocular therapy • Medical management
Medical Management • Beta-blockers • May delay aortic dilatation and progression to rupture or dissection. • The rate of surgical interventions has substantially declined during the past decade of beta-blockade use.
Medical Treatment • Anticoagulants are needed after artificial heart-valve placement • IV antibiotic therapy is required during cardiac and noncardiac procedures to prevent bacterial endocarditis • Progesterone and estrogen therapy have been used to induce puberty and reduce the patient's ultimate height - if tx is begun before puberty
Referrences • Caffey’s Pediatric Diagnostic Imaging, Vol. 2, Kuhn, Slovis and Haller, Mosby, 2004. • Thoracic Imaging, Webb, R. and Higgins, C., Lippincott Williams & Wilkins, 2005. • emedicine.com • mayoclinic.org • marfan.org