Download
1 / 15
240 likes | 785 Views
Next generation sequencing for breast cancer. Helen Lindsay Leeds DNA lab. Sanger sequencing. Targeted approach with each reaction representing a single PCR product (up to ~1kb) Analysis trace represents an average result from thousands of molecules Capacity up to ~1Mb/day.

E N D
Next generation sequencing for breast cancer Helen Lindsay Leeds DNA lab
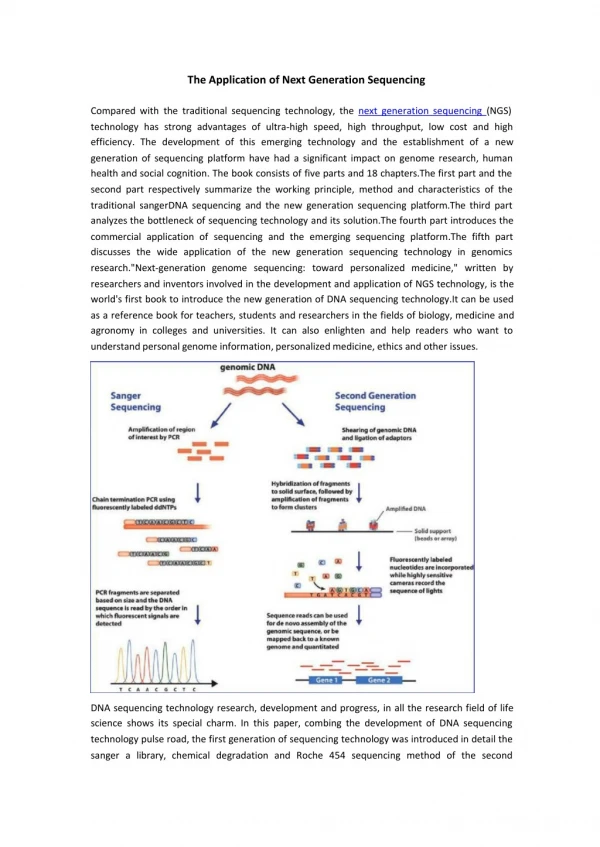
Sanger sequencing • Targeted approach with each reaction representing a single PCR product (up to ~1kb) • Analysis trace represents an average result from thousands of molecules • Capacity up to ~1Mb/day
BRCA screening: previous method • 15 patient panels set up every 10d • 40d turnaround time • For each panel: • Sanger sequencing of BRCA1 and BRCA2 • 10 x 96 well plates covering 59 amplicons • Tecan robots, M13 tagged primers, barcoding • protein truncation test – BRCA2 exon 11 (3x) • MLPA (2x) • any sequencing repeats and confirmations required • 1 lead scientist plus 3 technicians to cover workload
Second generation sequencing • Entire input sample is sequenced • Millions of small DNA fragments sequenced in parallel • Each sequence read represents a single starting DNA molecule • Capacity up to ~25Gb per day (~25,000x Sanger approach)
Clonal sequencing of BRCA • 20 patient panels set up every 10d • 40d turnaround time • For each panel: • clonal sequencing of BRCA1 and BRCA2 on Illumina GAIIx • MLPA (2x) • any confirmations/repeats required (Sanger sequencing) • 1 lead scientist plus 2 technicians to cover workload • Increase throughput, lower costs
Library preparation I • Target enrichment of BRCA1 and BRCA2: • long PCR of the complete CDS of BRCA1 and BRCA2 in 22 amplicons (1.2-5.8kb) • Shearing of pooled PCR products using the Covaris S2 instrument and verification using the Agilent Bioanalyzer
Library preparation II • End repair, A addition and ligation of tagged (6bp barcode) adaptors • Agarose gel size selection and gel extraction • Enrichment PCR and verification on the Agilent Bioanalyzer • Quantification and pooling of tagged samples
Cluster generation • Hybridise to flow cell • Bridge amplification • Cleave reverse strands • Hybridise sequencing primer
Sequencing • Copy template using fluorescently labelled, reversibly terminated nucleotides • Capture fluorescence signal after each incorporation step • Remove blocking group to allow addition of next base
Data analysis • Data analysis using NextGENe (SoftGenetics) software • conversion to appropriate format • remove low quality files • tag sorting • alignment to reference sequence • Generation of mutation reports • manual inspection to confirm variants and exclude artefacts • Generation of coverage information; custom spreadsheets automatically check coverage at each base over the region of interest • a minimum threshold of 50-fold coverage is required for diagnostic screening
Post analysis • Confirmation of all sequence variants other than known neutral polymorphisms by Sanger sequencing • Sanger sequencing of any regions with less than 50-fold coverage • Creation of a diagnostic report combining sequence data with MLPA results
Discussion • To date we have sequenced and reported ~300 patients, with a 10% pick-up rate of pathogenic mutations (excluding dosage abnormalities) • All mutations and UVs confirmed by Sanger sequencing • 100% concordance • 40% reduction in average test cost • 50% reduction in hand-on staff time • most significant reduction in sequence checking time • 30-40% reduction in consumables costs • Improvement in turnaround times
Future developments • Alternative enrichment techniques • high throughput long PCR • hybridisation based target capture • Automation of library preparation • Optimise protocol to detect dosage changes • More diseases • HNPCC in final stages of validation • potential for testing more genes in parallel
Acknowledgements • Leeds DNA lab • Nick Camm • Rachel Robinson • Ruth Charlton • Leeds Institute of Molecular Medicine • Heather Fraser • Jo Morgan • Graham Taylor