Download
1 / 12
120 likes | 440 Views
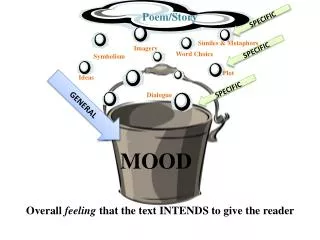
Mood stabilisers. At least: A treatment that is effective in augmenting the management of mania and/or depression without causing switching into the opposite pole Not toxic Ideally: Effective in preventing both mania and depression Useful in both the acute situation and in relapse prevention

E N D
Mood stabilisers • At least: • A treatment that is effective in augmenting the management of mania and/or depression without causing switching into the opposite pole • Not toxic • Ideally: • Effective in preventing both mania and depression • Useful in both the acute situation and in relapse prevention • Well tolerated to increase compliance
Olanzapine 1 • Has a bipolar license • Strongly anti-manic • Found to have mood elevating effects • Less potent than SSRI’s1, though Olanzapine plus fluoxetine demonstrated superior efficacy for treating resistant depression compared to either agent alone • Shelton RC et al. Am J Psych 158: 131-134
Olanzapine 2 • Further studies (open label, retrospective case note reviews and case reports) show the benefit of olanzapine in the treatment of depression1,2,3,4,5,6, both as monotherapy and in combination with SSRI’s • Conflicting evidence regarding metabolic effects: • Weight gain • Abnormal glucose metabolism • Raised cholesterol levels • Dube S et al. Biological Psychiatry 51(8 Suppl.) 66S. 2002 • Adli M et al. Nervenarzt 70(1): 68-71 • Tohen M. et al. European Neuropsychopharmacology 9 (Suppl. 5), S246. 1999 • Konig F et al. Neuropsychobiology 43(3), 170-4, 2001 • Rothschild AJ et al. Journal of Clinical Psychiatry 60(2), 116-8. 1999 • Shelton R et al. Schizophrenia Research 36 (1-3), 297-8. 1999
Lamotrigine (1) • Inhibition of Na channels, inhibit glutamate release • Clear evidence for efficacy in bipolar depression1 (licensed in 24 countries) • Studies underway suggestive of and seeking clarity for benefit in rapid cycling bipolar disorder1. Less evidence for efficacy in mania • Open studies & anecdotal reports of benefit in unipolar and treatment resistant depression2 • No risk of manic switching (highest with tricyclics) – a true mood stabiliser3 • Caution with dose escalation – rash • Macdonald KJ & Young LT. CNS Drugs (2002) 16(8): 549-62 • Barbee JG & Jamhour NJ. J Clin. Psych. (2002) 63(8) 737-41 • Calabrese JR et al. Am J Psych (1999) 156(7): 1019-23
Lamotigine – Any Mood Episode1 • Calabrese et al 2002
Lamotigine – Manic Episode1 • Calabrese et al 2002
Lamotigine – Depressive Episode1 • Calabrese et al 2002
Olanzapine • Therapeutic indications • Olanzapine is indicated for treatment of moderate to severe manic episode1 • In patients whose manic episode has responded to olanzapine treatment, olanzapine is indicated for the prevention of recurrence in patients with bipolar disorder1 • If a new manic, mixed, or depressive episode occurs, olanzapine treatment should be continued (with dose optimisation as needed), with supplementary therapy to treat mood symptoms, as clinically indicated 1. Zyprexa (olanzapine) Summary of Product Characteristics
In patients without psychotic features Primary measures: YMRS or remissions rates Olz vs Val3 weeks Olz vs Haloperidol6 weeks 0 60 -2 56.7%n=104 50 -4 40 -6 41.6%n=89 -8.69n=72 % Patients in remission 30 -8 Mean change in YMRS score -10 20 -14.11n=63 -12 10 -14 0 -16 p=<0.001 p=0.043 Olanzapine Haloperidol Val Ref (s) : Tohen M et al (2001) Poster presented at the APA, New Orleans 2001 Tohen M et al (2002) Am J Psychiatry 159: 1011-1017
Olanzapine Lithium Time to Relapse into Depression:Based on Symptomatic Rating Scale Criteria* 100 p=0.889 80 60 % probability ofremaining in remission 40 20 0 0 50 100 150 200 250 300 350 400 Time to relapse of depression (days) * HAMD-21 total score >15 Tohen M et al (2002).Presented at 3rd European Stanley Foundation Conference on Bipolar Disorder, Germany, 13 Sept. 2002
Source: Weight change Review: Reviewer Memo: Tohen M et al (2002).Presented at 3rd European Stanley Foundation Conference on Bipolar Disorder, Germany, 13 Sept. 2002 Slide Modified: Memo:
Source: Weight change Review: Reviewer Memo: *defined as 7% change from baseline over 52 weeks follow up Tohen M et al (2002).Presented at 3rd European Stanley Foundation Conference on Bipolar Disorder, Germany, 13 Sept. 2002 Slide Modified: Memo: