Download
1 / 35
360 likes | 544 Views
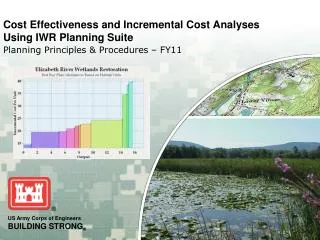
Subgroup Analyses: Can We ‘Smooth' out the Rough Edges?. Daniel Sargent, PhD Mayo Clinic Sept 28, 2006. Outline. Motivation Subgroups ARE medicine (especially its future) Examples Good and bad conduct Strategies Hierarchical models Smoothing approaches Conclusion.

E N D
Subgroup Analyses: Can We ‘Smooth' out the Rough Edges? Daniel Sargent, PhD Mayo Clinic Sept 28, 2006
Outline • Motivation • Subgroups ARE medicine (especially its future) • Examples • Good and bad conduct • Strategies • Hierarchical models • Smoothing approaches • Conclusion
Subgroups analysis: My Definition & My Bias • Definition: An effort to draw inference on an effect of an intervention in a set of patients smaller than the entire experimental cohort • Bias: Such inferences will be more robust when based on a model using all patients than an analysis restricted to just the cohort of interest
Subgroups are medicine • If all patients were the same, wouldn’t need physicians • Human Genome Project massively expanding knowledge base • Technology, biology, chemistry, etc. allowing manufacture of highly specific, targeted compounds • Patients seek ‘tailored’ treatment recommendations
Example: Colon Cancer: Model-Derived Estimates of 5 year DFS (%) with Surgery plus Adjuvant Therapy Gill, JCO 2004; http://www.mayoclinic.com/calcs
Example: Breast Cancer • Most common cancer in women in the US • The HER-2 gene is overexpressed in 25-30% of breast cancers; associated with worse prognosis. • Trastuzumab, a humanized monoclonal antibody targets the HER-2 receptor; previous trials have demonstrated activity in the treatment of HER-2 overexpressing late stage breast cancer. • Performed a clinical trial testing trastuzumab in subset of HER-2 positive women with early stage breast cancer
Disease-Free Survival Survival AC→T+H →H 62 events AC→T+H →H 134 events AC→T 92 events 94% AC→T 261 events 91% 87% 92% 85% 87% 75% HR=0.48, 2P=3x10-12 HR=0.67, 2P=0.015 67% Years Years Romond et al, NEJM 2005
Avoiding subgroup analysis: Targeted Phase II/III Trials Patient Selection for targeted therapies • Test the recommended dose on patients who are most likely to respond based on their molecular expression levels • May result in a large savings of patients (Simon & Maitournam, Clinical Cancer Research 2004)
Trials in targeted populations • Gains in efficiency depend on marker prevalence and relative efficacy in marker + and marker – patients • Details: Session #13 tomorrow (Simon & Maitournam, CCR 2004)
Case Study: Stage II colon cancer • Colon cancer: Prognosis defined by stage • Prior trials generally enrolled patients with both stage II and III disease • Previous randomized trials uniformly demonstrate benefit of chemotherapy in stage III patients (node positive) • Previous trials & pooled analyses mixed regarding benefit in stage II patients • No single trial powered for modest effect seen in stage II ( ↑ 2-3% in 5 year survival)
Meta-analysis Stage II Adjuvant Therapy N=2,732 RR=0.88 P=0.08 Benson et al. J Clin Oncol. 2004
American Society of Clinical Oncology Guidelines 2004 • Direct evidence from randomized trials does not support routine use of chemotherapy for patients with stage II colon cancer. • Those who accept the relative benefit in stage III disease as adequate indirect evidence of benefit for stage II disease are justified in considering chemotherapy, particularly for patients with high-risk stage II disease. • Ultimate clinical decision should be based on discussions with the patient. Benson et al. J Clin Oncol. 2004
R New therapy: FOLFOX FOLFOX4: LV5FU2+ oxaliplatin 85 mg/m² N=2246 Stage II: 40% Stage III: 60% LV5FU2 Primary end-point: disease-free survival (DFS) de Gramont et al., ASCO 2005
Disease-free Survival (ITT) 1.0 0.9 0.8 6.6% 0.7 0.6 Events FOLFOX4 279/1123 (24.8%) LV5FU2 345/1123 (30.7%) HR [95% CI]: 0.77 [0.65–0.90] DFS probability 0.5 0.4 0.3 p<0.001 0.2 0.1 0.0 0 6 12 18 24 30 36 42 48 54 60 66 Months de Gramont et al., ASCO 2005
Disease-free Survival (ITT) Stage II and Stage III Patients 1.0 0.9 3.5% 0.8 0.7 8.6% 0.6 DFS probability 0.5 0.4 0.3 FOLFOX4 – 451 Stage II LV5FU2 – 448 Stage II FOLFOX4 – 672 Stage III LV5FU2 – 675 Stage III HR [95% CI]: 0.82 [0.60–1.13] Stage II 0.75 [0.62–0.89] Stage III 0.2 0.1 0.0 0 6 12 18 24 30 36 42 48 54 60 66 Months Data cut-off: January 16, 2005 de Gramont et al., ASCO 2005
DFS in high-risk* stage II patients 1.0 0.9 5.4% 0.8 Probability 0.7 HR 0.76 FOLFOX4 – 286 HRStage II LV5FU2 – 290 HR Stage II 0.6 0 6 12 18 24 30 36 42 48 DFS (months) • *T4 and/or bowel obstruction and/or tumor perforation and/or poorly differentiated tumor and/or venous invasion and/or <10 examined LNs • Data cut-off: January 16, 2005 de Gramont et al., ASCO 2005
FDA Action • Approval of FOLFOX therapy only in stage III patients, even though trial designed for stage II and III patients • Possible rationale • Standard chemotherapy vs control not shown beneficial in stage II patients • This trial not significant for experimental vs standard chemotherapy
Stage II trial: QUASAR R A N D O M I Z E Observation (n = 1617) • Colon or rectal cancer • Stage I-III • Complete resection with no evidence of residual disease No clear indicationfor chemotherapy (n = 3239) Chemotherapy (n = 1622)* Gray et al. ASCO 2004. Abstract 3501. At: http://www.asco.org/ac/1,1003,_12-002511-00_18-0026-00_19-0010698,00.asp. Accessed November 2004.
QUASAR: Overall Survival 100 Observation (n=1622) Chemotherapy (n=1617) 80 60 % of Patients 40 P = .02 5-year OS, Observation = 77.4% vs Chemotherapy = 80.3% Relative risk = 0.83 (95% CI, 0.71-0.97) 20 0 0 1 2 3 4 5 6 7 8 9 10 Years Gray et al. ASCO 2004. Abstract 3501. At: http://www.asco.org/ac/1,1003,_12-002511-00_18-0026-00_19-0010698,00.asp.Accessed November 2004.
Implication: Stage II patients • Compared to control, 5-FU provides 2-3% ↑ in OS, statistically significant in a single trial • Debate over clinical relevance • In a large trial, FOLFOX provides 3-4% ↑ in DFS compared to 5-FU, not statistically significant for stage II alone • No hint of interaction between rx and stage, p = 0.77 • On its own, debatable benefit compared to 5-FU • Cross trial comparison: FOLFOX may result in 5-7% improvement vs control, but not approved • No debate about clinical relevance Grothey & Sargent, JCO 2005
Stage II Colon Cancer: Lessons Learned • Decisions based on subgroups may seem rational at the time, but lead to unintended consequences • Results may make further trials impossible (FOLFOX vs control) • Need better approaches to analyze subgroups using modeling (or meta-analyses), not individual trial results
Potential solution for prospectively defined subgroups: Hierarchical models • Goal: Test a treatment in a number of populations • Hypothesis: Effect may depend vary between populations • Example: Targeted cancer therapy • Mechanism of action based therapy • Multiple tumor types express ‘target’, to varying degrees
Basic statistical formulation • Suppose N subgroups, with mean response mi, i=1,...N • Assume mi ~ N(m,s2) • If Bayesian, put a prior on s2 • Depending on estimate of s2, allows heterogeneity between subgroups • Easily extends to non-normal models
Hierarchical Model: Example • Phase II clinical trial of a new agent specifically targeted at patients with a methylated MGMT promoter • Prevalence from 10% to 60% across various cancer types • High prevalence seen in Head and Neck, Esophageal, Colorectal, and Non Small-Cell Lung Cancer • Goal: Determine if overall efficacy > 10%, but efficacy may depend on tumor type
Logistic regression Example • Hierarchical logistic model for tumor response • Stopping rules for each tumor site • P ( Response ratei > 10%) < 10% OR • P (Response ratei > 10%) < 25% & P (Response rateOverall > 10%) < 10% • Simulation for operating characteristics • Benefits • Single trial (opposed to 4) • Use all data formally but flexibly
Survival Example • Survival following chemotherapy for colon cancer • Pooled analysis of 5 trials, suggestion of a study-specific treatment effect (a different type of subgroup) • Fit a random effect Cox model • l(t; x) = l0i(t) exp (xmi) • mi ~ N(m,s2) • Can either model l0 parametrically, or use Cox model
Model Results Prior mean for precision (1/s2) = 50, posterior mean 106, Little evidence of heterogeneity Sargent et al, 2000
Another approach: Modeling Interactions using Shrinkage • Subgroup analyses are fundamentally looking at interactions • In multi-factor experiment, the number of interactions can explode • Well known that shrinkage (or model averaging) provides much better performance than all or nothing approach (stepwise) • Idea: Include interactions in model, but shrink them away if they are not strongly supported by the data
Another approach: Modeling Interactions using shrinkage • Dental Experiment • Dentures are often made with a soft liner between the gums and the hard denture base • Polishing the liner can cause a gap between the liner and the base • Such gaps harbor pathogens like Candida • The experiment • Main interest: new vs. standard soft liner material • Factor M: 2 materials • Factor P: 4 polishing methods • Factor F: 8 finishing methods • Fully crossed design, no replication • Outcome measure: gap btwn liner & base, in log10 mm Pesun, Hodges & Lai (2002) J. Prosthetic Dentistry
Smoothing interactions: Smoothed ANOVA • Fit full ANOVA model (include all interactions) • y = XQ + e • y is 64 x 1, contains log10 gap • e is 64 x 1, normal mean 0, precision h0I64 • X is 64 x 64 • Q is 64 x 1; we will smooth/shrink its elements • 12 main effects, 52 interactions • Model interactions • qk ~ N (0,1/ fk) , k=13, …, 64 • Large fk implies qk shrunk toward 0
Smoothed ANOVA: The model/prior for the fk • How to model the interactions • Each interaction smoothed by its own fk • Each effect's fk are all the same, feffect • All two-way interactions are smoothed by a single f • Mix the above options • Use priors on fk to specify desired operating characteristics for interactions
Use Degrees of Freedom to set priors for the fk • Hodges & Sargent (2001 Biometrika) extended methods for computing DF in standard ANOVA to linear hierarchical models • Hodges et al (Technometrics, 2006) present methodology to use DF to set priors • Example: I want the 51 2-way interactions to share 5 degrees of freedom • See references for technical details • Ongoing work: extending to non-linear (Cox) models
Summary: Smoothed ANOVA • Subgroup analyses are fundamentally looking at interactions • A priori have low probability of a significant interaction, but don’t want to exclude the possibility • Idea: Include interactions in model, but shrink them
Summary • Subgroup analysis is essential to clinical research • People usually perform such analyses with best of intentions • Up-front thought can allow us to • Carefully define population under study • Pre-specify sub-populations to be examined • Hierarchical/Shrinkage models offer attractive possibilities for addressing subgroups, if defined prospectively
Thank You • Acknowledgements • Smoothed ANOVA: Jim Hodges • Colon Cancer: Axel Grothey, Aimery deGramont, Sharlene Gill