Download
1 / 41
410 likes | 625 Views
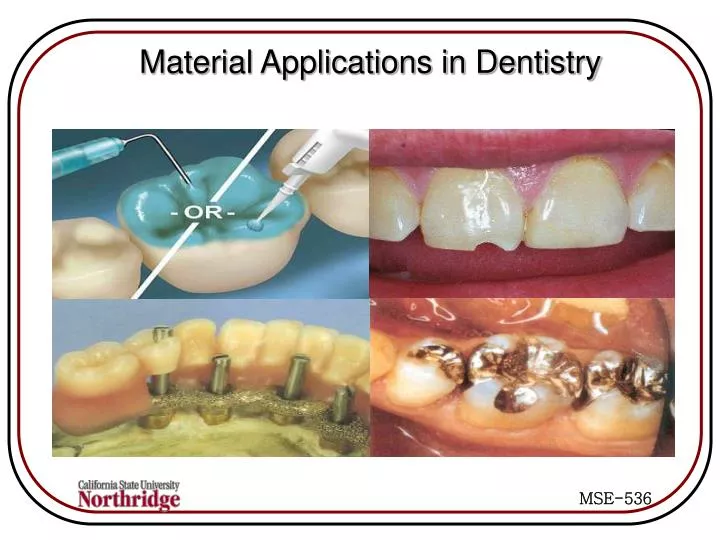
Material Applications in Dentistry. The mouth is a hostile environment: Large swings in temperature, pH High levels of bacteria High stresses, fatigue, corrosion. Synthetic Biomaterial Classes.

E N D
The mouth is a hostile environment: • Large swings in temperature, pH • High levels of bacteria • High stresses, fatigue, corrosion
Synthetic Biomaterial Classes • METALS: Co-Cr alloys, Stainless steels, Gold, Titanium alloys, Vitallium, Nitinol (shape memory alloys). Uses: Implants, orthodontics, reconstruction • CERAMICS: Alumina, Zirconia, Porcelain Uses: dental reconstruction. • COATINGS: Bioglasses, Hydroxyapatite, Diamond-like carbon, polymers. • POLYMERS: Resin matrix (bisphenol A-glycidyl methacrylate, BISMA), urethane dimethacrylate (UDMA) and inorganic fillers such as silicon dioxide silica.
Vitallium is a trademark for an alloy of 60% cobalt, 20% chromium, 5% molybdenum, and traces of other substances. The alloy is used in dentistry because of its light weight and resistance to corrosion. • Nitinol (50/50 Nickel-Titanium is a shape memory alloy that undergoes strain- and thermally-induced phase transformations
Implant Factors • Bulk properties: chemical composition, structure, purity and presence of leachables. • Surface properties: smoothness, COF, geometry, hydrophilicity, and surface charge • Mechanical properties: match properties of component being replaced, such as elastic modulus. Stability and fixation. • Long-term structural integrity: design for fatigue and fracture loading, wear, creep, plastic deformation, and stress corrosion cracking
Dental Implants Implants provide ways to anchor reconstructive dental appliances
Implants require two surgeries: • To place the implant in the bone, cover, and allow up to 6 months to heal • To uncover to expose post and finish the restoration
Fillings: Composite Amalgams Noble metals Gold Caps: Porcelain Polymer Composite
Dentistry in England Before After
ADHESIVE DENTISTRY Indications • Replace carious and fractured tooth structure. • Fill erosion or abrasion defects in cervical areas. • Correct unaesthetic shapes, positions, dimensions, or shades. • Bond silver amalgam restorations. • Cement crowns.
Mechanical interlocking by a cement to tooth dentin. Voids at interface limit strength and toughness Section through a femur after removal of stem of hip prosthesis showing mechanical interlocking by bone cement into cancellous bone Leakage of oral fluids and bacteria around dental filling material in tooth crown.
Diagrammatic representation of setting of zinc polyacrylate and bonding to a calcific surface. Structures of methyl cyanoacrylate and methyl methacrylate
Sealants Etch Apply sealant Cure
Glass-ionomers Most commonly referred to as glass ionomer cements (GIC's). • These are materials which consist of an aqueous polyacrylate and a fluoroaluminosilicate glass. • These set by an acid-base reaction in the presence of water. • These cements appear to adhere to tooth structure by formation of ionic bonds as a result of chelation of the carboxyl groups in the acid with the calcium and/or phosphate ions in the apatite of enamel and dentin.
COMPOSITION POWDER = CALCIUM FLUOROALUMINOSILICATE GLASS • Silicon 13.3% Phosphorus 2.5% • Aluminum 13.3% Fluoride 22.7% • Calcium 17.3% Oxygen 28.0% • Sodium 1.6% • LIQUID = POLYACRYLIC ACID OR • COPOLYMER OF ACRYLIC ACID • WATER
Most Common Dental Resin bisphenol A glycol dimethacrylate triethylene glycol dimethacrylate
BONDING MICRO-FILLED HYBRID RESIN Shake the Self-Etching Primer bottles, then dispense one drop each into dispensing dish and mix for 5 seconds. Apply to tooth surface. Light-cure for 20 seconds Using a VLC Curing Light. Apply thin layer to prosthesis with micro-tip. Light-cure each surface for 20 seconds. Hold for 1 minute. Light-cure for 1-2 seconds; then remove excess. Apply LINKMAX to primed porcelain surface. Dispense LINKMAX and mix for 10 seconds.
Composite Primer LINKMAX Self-Etching Primer MFR Hybrid Resin Inlay Composite Primer LINKMAX Self-Etching Primer
BONDING PORCELAIN Dispense one drop each Ceramic Primer into dispensing dish and mix for 5 seconds. Apply to bonding surface and dry. Shake the Self-Etching Primer bottles, then dispense one drop each into dispensing dish and mix for 5 seconds. Apply to tooth surface. Apply etchant, after 30 seconds, rinse with water and dry. Hold for 1 minute. Light-cure for 1-2 seconds; then remove excess. Light-cure each surface for 20 seconds. Apply LINKMAX to primed porcelain surface. Dispense LINKMAX and mix for 10 seconds.
BONDING PORCELAIN • Etchant Etchant • • Ceramic Primer Ceramic Primer • LINKMAX LINKMAX Self-Etching Primer Self-Etching Primer Porcelain Inlay Ceramic Primer Etchant LINKMAX Ceramic Primer LINKMAX Self-Etching Primer Self-Etching Primer Porcelain Veneer Etchant
BONDING METAL PROSTHESIS TO TOOTH STRUCTURE Metal Primer II Metal Crown LINKMAX Self-Etching Primer
The future • Adhesive dentistry • Improving the properties of adhesive materials. e.g. wear resistance, strength • Biocompatible materials • Antibacterial, bioactive, drug delivery • Increasing use of implants • Shorter healing periods • Poorer quality bone • Less bone • Growing natural teeth
Dental enamel is the hardest tissue in the body. It cannot regenerate itself, as the portions of the cell that generate it are lost by the time the tooth appears in the mouth. Research is under way to grow artificial enamel, or even whole teeth, using culturing and transplantation techniques. Challenge: How to produce, in culture, sufficient numbers of enamel forming cells. Approach: Grow cells on a scaffold. A team of researchers from the Institute of Medical Science at the University of Tokyo, reports that extracted epithelial cells from the developing teeth of a 6-monty-old pig continue to proliferate when they are cultured on top of a special feeder layer of cells, know as the 3T3-J2 cell line. This step boosts the number of dental epithelial cells available for enamel production. Seed the cultured dental epithelial cells onto collagen sponge scaffolds, along with cells from the middle of the tooth (dental mesenchymal cells). Transfer the scaffolds into the abdominal cavities of rats, where conditions were favorable for the cells in the scaffolds to interact and develop. When removed after 4 weeks, the remnants of the scaffolds were found to contain enamel-like tissue. Even after the multiple divisions that occurred during propagation of the cells in culture, the dental epithelial cells retained the ability to produce enamel, as long as they were later provided with an appropriate environment. Now that dental epithelial cells can be propagated in culture, the next step will be to achieve the same success with their partners in tooth formation, the dental mesenchymal cells. Further development of this technique will be aimed toward production of tissue to replace damaged or missing enamel, and ultimately, regeneration of whole teeth.
Tissue Reconstruction • Current strategies for jaw reconstruction require multiple procedures, first to repair the bone defect to offer sufficient support, and then to place the tooth implant. • Procedure can be painful and time-consuming, and the desired aesthetic and functional repair can be achieved only when both steps are successful. • Although the patient's quality of life can be improved significantly, the prognosis is often unpredictable, especially in young patients, whose jaws continue to grow, while the implant remains fixed.
The ability to bioengineer combined tooth and bone constructs, which would grow in a coordinated fashion with the surrounding tissues, could potentially improve the clinical outcomes, and also reduce patient suffering. • Under the guidance of Dr. Pamela C. Yelick, a research team at Tufts University (Boston, MA) has examined the feasibility of simultaneously reconstructing both teeth and bone. In 2002, the group first reported the regeneration of tooth crowns, from cultured tooth bud cells seeded onto biodegradable scaffolds and implanted into rat hosts. The morphology of the developing tissue-engineered tooth crowns closely resembled that of naturally formed teeth.
Next, they generated a hybrid tooth-bone construct, by combining a bone-marrow-derived stem-cell-seeded scaffold with the previously used tooth model, implanted and grown in the omenta (tissues connecting abdominal structures) of rat hosts. In this case, the formation of not only the tooth crowns but also tooth root and surrounding alveolar bone was observed. However, since the omentum offers an environment quite distinct from that of the natural tooth site, the jawbone, the team examined hybrid tooth-bone construct development using third molar tooth bud cells and bone marrow derived from, and implanted back into, the same minipig.
Their results showed the formation of organized bioengineered dental tissues closely resembling those of naturally formed teeth, including dentin, enamel, pulp, and periodontal ligament, after 12 weeks of implantation. • Further analyses confirmed the expression of tooth- and bone-specific markers on the bioengineered tissues. In addition, they observed novel mineralized tissue interface formation, including enamel/bone and dentin/bone interfaces. These results demonstrate the feasibility and therapeutic potential for regenerating tooth and bone from autologous stem cells, for craniofacial reconstructions in humans. This model is currently being modified to improve alveolar bone formation, regenerated dental tissue orientation, tooth root development, and tooth eruption.
Protein Implants to Stimulate the Growth of Lost Tissue • Titanium dental implants coated with proteins that induce bone formation may be a key advancement in treating tooth loss due to gum disease, researchers say. • In laboratory tests, Medical College of Georgia (MCG) researchers applied a protein onto implants that directs endogenous stem cells to become bone-forming cells. The result was a nearly complete regeneration of lost tissue. Loss of teeth and bone is a common and devastating result of gum disease.
regeneration requires two characteristics: a stable wound and space for the regenerated tissue to grow during the initial stages of healing. This often begins within a week or two. • Researchers found that some materials may actually hinder tissue regeneration. For example, hydroxyapatite particles, which are chemically similar to the mineral component of bone, may actually interfere with regeneration because they may not resorb quickly enough and may block the space for new tissue to grow into.”
Proteins that direct stem cells to become bone-forming cells, called bone morpheonetic proteins, have already shown promise as a regeneration therapy for craniofacial reconstruction. • Proteins were placed around teeth in animal test subjects. The bone-forming cells grew into existing bone and eventually morphed into bone themselves. However, the root of the tooth was destroyed by the replacement bone. That process impeded regeneration of other essential tissues around the tooth.
Applying the protein to implants displayed almost complete regeneration. The generated bone bonded with the implant’s surface and, eventually, existing bone in the gums, allowing the regeneration of gum tissues. • The next step is clinical trials of an implant coated with the proteins.



![[PDF READ ONLINE] Materials in Dentistry: Principles and Applications](https://cdn7.slideserve.com/12501566/slide1-dt.jpg)
