Download
1 / 43
460 likes | 645 Views
The Respiratory System. Chapter 18. Operations. Pulmonary ventilation Moving air in & out External respiration Gas exchange between alveoli & blood Internal respiration Gas exchange between blood & cells. Helps pH control. Anatomical Components. Upper respiratory tract nose, pharynx

E N D
The Respiratory System Chapter 18
Operations • Pulmonary ventilation Moving air in & out • External respiration Gas exchange between alveoli & blood • Internal respiration Gas exchange between blood & cells Helps pH control
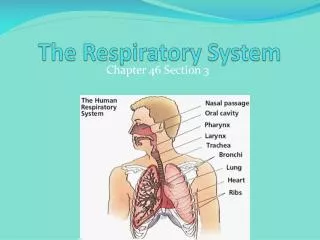
Anatomical Components • Upper respiratory tract nose, pharynx • Lower Respiratory System Trachea, larynx & bronchi & lungs • Conducting zone = tubing • Respiratory Zone= Gas exchange Bronchioles, alveolar sacs & alveoli
Nose • Nose: external nares nasal cavity internal nares Nasal septum splits in two Nasal conchae swirl air over mucus membrane • Designed to: Filter, Warm, Humidify • Trap dust and infectious agents • Detect olfactory stimuli • Modify vocal sounds
Pharynx • Funnel shaped tube from internal nares to larynx = “throat” • Upper = naso pharynx • Middle = oropharynx Between uvula & top of epiglottis • lower = laryngeal pharynx Connects with both esophagus & larynx Thus both air & food & drink
Larynx • Short tube of cartilage • Thyroid cartilage- anterior = “Adam's apple” • Epiglottis – upper leaf-shaped piece During swallowing larynx moves up and epiglottis covers opening to trachea • Cricoid cartilage- forms inferior wall • Paired arytenoids- above cricoid attach to vocal cords & pharyngeal muscles
Voice Production • Mucous membrane of larynx two pairs of folds • Upper = false vocal cords • Lower = true vocal cords Contain elastic ligaments stretched between cartilage Move out into air way and vibrate Pitch adjusted by tension and diameter of ligaments
Trachea • Trachea- larynx upper part of T5 vertebra R. & L. primary bronchus Lined with pseudostratified ciliated mucous membrane dust protection – move toward pharynx • C-shaped cartilage rings keep lumen open
Bronchi & Bronchioles • Bronchi also contain cartilage rings • Primary bronchi enter the lungs Blood vessels, lymphatic vessels & nerves enter lungs with bronchi • In lungs branch secondary bronchi one for each lobe of lung • tertiary bronchi terminal bronchi • Smaller bronchi have less cartilage and more smooth muscle ANS can adjust diameter = resistance to flow
Lungs • Two organs (R. & L) • Surrounded by pleural membrane Parietal pleura attached to diaphragm & thoracic wall Visceral pleura attached to lungs Between is pleural cavity filled with fluid Broad bottom = base; Pointy top = apex • Right lung has 3 lobes • Left lung has 3 lobes & cardiac notch
Lung Lobes • Divided in lobules fed by tertiary bronchus • Further divisions terminal bronchiole • respiratory bronchiole Lined with non-ciliated cuboidal epithelium • alveolar ducts alveolar sacs
Alveoli • Cup-shaped out pouch of sac Lined with thin alveolar cells (simple squamous) • Scattered surfactant secreting cells Lowers surface tension & humidifies • Alveolar macrophages- “cleaners” • Gases diffuse across combined epithelia of alveolus & capillary • Combination called: Respiratory Membrane
Pulmonary Ventilation • Air flows between atmosphere & lungs due to difference in pressure Caused by respiratory muscles • Inhalation: diaphragm & external intercostals Diaphragm contracts lung volume • Lung moves due to seal between parietal & visceral plura
Exhalation • Resting exhalation due to muscle relaxation= passive process Diaphragm rises & ribs fall lung volume • Can be active using internal intercostals & abdominal muscles Push diaphragm up & pull ribs in More lung volume
Pressure Changes • lung volume alveolar pressure • Atmospheric pressure is constant • Atmospheric > alveolar inhalation • During exhalation lung rises • Alveolar> Atmospheric exhalation
Air Flow Terms • Frequency (f) = breaths per minute Normal ~12 breaths per min • Tidal volume (TV) = volume moved in one breath Normal ~ 500 ml • Minute Ventilation (MV) = f x TV • ~ 70% of TV reaches alveoli (350 ml) Only this involved in gas exchange • 30% in airways = Anatomic Dead Space
Lung Volumes • Inspiration beyond resting = Inspiratory reserve volume • Expiration beyond resting (active) = Expiratory reserve volume • Air left after a maximum expiration = residual volume
Lung Capacities • Inspiratory capacity= TV + inspiratory reserve • Functional residual capacity = Residual volume + expiratory reserve • Vital capacity (VC) = Expiratory reserve + TV + Inspiratory reserve • Total lung capacity = VC + residual
Breathing Patterns • Eupnea = normal breathing Highly variable in pattern • Special modifications for speech and emotional responses • Also variations fro coughing & sneezing to clear airways See table 18.1
Nature of Air • Mixture of gases (N2, O2,, CO2, H2O & others) • Each gas has own partial pressure (Px) • Each gas diffuses down partial pressure gradient • Total = sum of partial pressures = atmospheric pressure
Pulmonary Gas Exchange: External Respiration • O2 diffuses from air (PO2 ~105mm Hg) incoming blood (PO2 ~40mm Hg) • Continues until equilibrium (PO2 ~105mm Hg) Some unexchanged mixture in out flow so Arterial blood is ~100 mmHg • Meanwhile blood (PCO2 ~45) diffuses to alveolar air (PCO2 ~40) Again to equilibrium
Systemic Gas Exchange: Internal Respiration • Occurs throughout body • O2 diffuses from blood to cells • PO2 lower in cells because of use • Meanwhile CO2 diffuses in opposite direction
Transport of Oxygen • O2 dissolves poorly 98.5% bound to hemoglobin in RBCs Binding depends on PO2 High at lung and lower at tissue PO2s • Tissue release of O2 increased by: High CO2 Acidity Higher temperatures
Transport of Carbon Dioxide • As comes in to blood from cells • Some dissolved (7%) • Bound to proteins including Hemoglobin (23%) • Becomes bicarbonate ions (70%) CO2 + H2O <=> H+ + HCO3- • Process reverses at lungs
Control of Respiration • Medullary respiratory area in medulla Contains both inspiratory & expiratory areas • Quiet breathing: inspiratory area nerve signals to inspiratory muscles for ~2 sec inspiration Then becomes inactive & muscles relax Expiration Expiratory centre active only during forceful breathing • Area in pons adjusts length of inspiratory stimulation
Regulation of Respiratory Center • Cortical input: voluntary adjustment of patterns Protection & talking Chemoreceptor input will override breath-hold • Chemoreceptor input Central receptors in medulla Peripheral receptors in arch of aorta respond to increased H+ or PCO2increased ventilation • Thus negative feedback loop to maintain blood & brain pH • Significant falls in PO2 also stimulates breathing
Other Regulatory Factors • Limbic system- anticipation of activity or emotion can stimulate • Proprioception stimulates on start of activity • Temperature warming increases • Pain- Sudden pain apnea Prolonged somatic pain can increase rate • Airway irritation cough or sneeze • Inflation reflex- bronchi wall stretch receptors inhibit inspiration Prevents overinflation
Aging • Everything becomes less elastic • Decrease in Vital capacity • Can decrease blood O2 level • Decreased exercise capacity • Decreased macrophage activity • Increased susceptibility to pulmonary disease