Download
1 / 34
350 likes | 775 Views
Self-Regulating Oxygen Delivery System. Advisors: Dr. Debatosh Debnath Dr. Cheryl Riley-Doucet. Lauren Ehardt Katelyn Klein Jason Nixon. Outline. Introduction Problem Goals Background Benefits of Automatic Control System Design Future Plans. Introduction.

E N D
Self-Regulating Oxygen Delivery System Advisors: Dr. Debatosh Debnath Dr. Cheryl Riley-Doucet Lauren Ehardt Katelyn Klein Jason Nixon
Outline • Introduction • Problem • Goals • Background • Benefits of Automatic Control System • Design • Future Plans
Introduction • Supplemental oxygen is one of the most widely used therapies for people admitted to the hospital • One million COPD patients in US • Manual oxygen control is the norm [NHLBI, 2006] Who is this?
Need for Automatic Control • No device exists to automatically regulate oxygen flow to a patient
Neonatal Environment • Manual control of oxygen delivery • Patient to nurse ratio is high • Lack of awareness: effects of hyper-oxygenation [Firestone, 2007] http://news.thomasnet.com/images/large/498/498329.jpg
Outpatient Setting • Difficult to prescribe oxygen flow rates • Oxygen levels vary • Activity level • Environment • No set standard to determine oxygen flow rate [Pilling, 1999] [Guyatt, 2000]
Project Goals • Design a self-regulating device • Control oxygen flow based on SpO2 readings • Automatically adjust valve opening based on pulse oximeter signal
Project Goals (contd.) • Device features • Safe • Reliable • Easy to use • Customizable • Portable • Cost-effective
Oxygen Therapy: Background • Oxygen saturation • Oxygen therapy patients • Hyper-oxygenation • Mechanisms of oxygen therapy • Current research
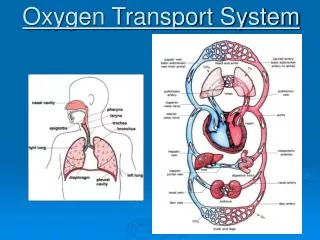
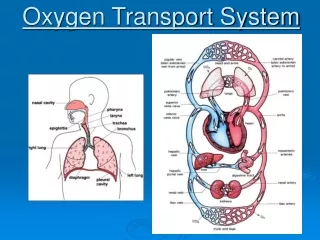
Oxygen Saturation of Blood • Why do we need oxygen? • Measured as percentage: Oxygen Saturation of Arterial Blood: SaO2 = true oxygen saturation SpO2 = measured by pulse oximeter • Normal adult SaO2 = 97-99% • Hypo-oxygenation: SaO2 < 90% • Normal infant SaO2 = 86-92% [Schutz, 2001] [Woods, 2005]
Oxygen Therapy Patients • Adults suffering from respiratory failure • Chronic obstructive pulmonary disease (COPD) • Pneumonia • Asthma • Treatment: Long term oxygen therapy (LTOT) • Neonates • Supplemental oxygen is most common form of therapy [Pilling, 1999]
Hyper-oxygenation • CO2 retention • Neonates • Lung toxicity • Brain toxicity • Retinopathy of prematurity (ROP) [Mack, 2006] www.cartage.org.lb/.../humrespsys4.gif
Stevie Wonder Suffered from Retinopathy of Prematurity
Mechanisms of Oxygen Therapy • Low flow delivery systems (0-15 lpm) • Variable performance • Nasal canulla and face masks • High flow delivery systems (>15 lpm) • Fixed performance • For respiratory assistance in addition to supplemental oxygen [McGloin, 2007] www.jsdobbs.ie/jsdobbs/Main/Products_Oxygen.htm
Mechanisms of Oxygen Therapy (contd.) • Three oxygen sources • Liquid Oxygen • Oxygen Cylinder • Oxygen Concentrator http://www.waldosworld.org/gallery03/oxygentank.jpg [sunzi1.lib.hku.hk/hkjo/view/21/2100807.pdf ]
Mechanisms of Oxygen Therapy (contd.) • Oxygen flowmeter • Controls oxygen flow rate • Oxygen blender • Controls oxygen concentration and flow rate • Mixes oxygen and air http://www.gehealthcare.com/usen/suction_oxygen/oxygen_therapy/images/blender_c_l.jpg
Mechanisms of Oxygen Therapy (contd.) • Measuring oxygen saturation • Pulse oximetry • Non-invasive • Oximeters use alarms www.medisave.co.uk/images/nonin-3100-pulse.jpg [Kamat, 2002]
Current Research • Columbia Life Systems • SmartBlender™ [http://smartblender.com/index.html] • Saturation Driven Oxygen Therapy (SDOT) • Computer simulation shows automatic control is more effective in maintaining constant SpO2 than manual control • Hospitals are switching to oxygen blenders [Iobbi, 2007]
Benefits of Automatic Control • Automatic adjustment of oxygen delivery • Increases amount of time patients spend in desired SpO2 range • Decreases hypo-oxygenation events [Zhu, 2005]
Benefits (contd.) • Avoid fluctuations in SpO2 • Prevent severe ROP • Improve quality of care • Lessen nurse workload • Fewer alarms • Prevent inappropriate action to reduce alarms [Zoidis, 2007]
HCS12 Microcontroller • Program in C • Runs up to 25 MHz • Pulse width modulation (PWM) controls current to the proportional valve • Serial communication interface (SCI) receives data from pulse oximetry board
Pulse Oximeter Sensor • Two LEDs emit red and infrared wavelengths of light through skin • Hb absorbs red wavelengths • HbO2 absorbs infrared wavelengths • Photodetector on other side picks up intensity of transmitted light • SpO2 is calculated by analyzing received light • Utilizes cardiac pulse to distinguish arterial blood from other mediums Hb = hemoglobin not bound to oxygen HbO2 = hemoglobin bound to oxygen
Pulse Oximetry Board • Low power • Data outputs: SpO2 and pulse rate • Eight second average (or instantaneous) • Serial communication BCI OEM 31392B1 Board
Parker Proportional Valve • Controls the flow based on input voltage • PWM generates variable input voltage • Oxygen safe Parker Valve
Cost Analysis Blenders cost $1000+ Project Total: $352
Progress • Literature reviews • 50+ research articles • Visited respiratory therapist at Crittenton Hospital • Researched valves and oximeter boards from many manufacturers • Finished introduction of paper • Started learning HCS12 modules
Progress (contd.) • Received valve • Received oximeter board • Purchased oxygen tubing from Crittenton Medical Equipment store • Flow meter from Binson’s • Purchased helium tank • Continue learning HCS12 modules
Final Goals • Working prototype by July 16th • Finish paper • Create poster
Acknowledgement We thank Kristen Munyan of Beaumont Hospital for introducing us to the problem and Steve Yax of Crittenton Hospital Medical Center for answering our questions on respiratory equipment. This work was supported in part by the Bioengineering and Bioinformatics Summer Institutes Program of the National Institutes of Health and the National Science Foundation under grant 0609152.
References • T. Croxton, “HLBI and CMS launch large study of home oxygen therapy for COPD,” NIH News, NHLBI Communications Office, 2006. • K. Firestone and H. Adams, “Evidence-based oxygen therapy for very low birth weight infants,” Journal of Pediatric Nursing, vol. 22, no. 2, p. 145, 2007. • G. H. Guyatt, et al., “Appropriateness of domiciliary oxygen delivery,” Chest, vol. 118, pp. 1303-1308, 2000. • D. L. Woods, “Newborn care manual,” Unit 26, International Association for Maternal and Neonatal Health, 2005. • J. Pilling and M. Cutaia, “Ambulatory oximetry monitoring in patients with severe COPD: A preliminary study,” Chest, vol. 116, pp. 314-321, 1999. • E. Mack, “Oxygen administration in the neonate,” Newborn and Infant Nursing Reviews, vol. 6, no. 2, pp. 63-672, 006. • S. L. Schutz, “Oxygen saturation monitoring by pulse oximetry,” AACN Procedure Manual for Critical Care, vol. 4, pp 77-82, 2001.
References (continued) • Z. Zhu, et al., “Continuous oxygen monitoring- better way to prescribe long-term oxygen therapy,” Respiratory Medicine, vol. 99, pp. 1386–1392, 2005. • S. McGloin, “Administration of oxygen therapy,” Nursing Standard, vol. 22, no. 21, pp. 46-48, 2008. • V. Kamat, “Pulse oximetry,” Indian Journal of Anaesthesia, vol. 46, no. 4, pp. 261-268, 2002. • M. G. Iobbi, A. K. Simonds, and R. J. Dickinson, “Oximetry feedback flow control simulation for oxygen therapy,” Journal of Clinical Monitoring and Computing, vol. 21, pp. 115–123, 2007. • D. Zoidis, “Retinopathy of prematurity: latest evidence regarding the use of supplemental oxygen,” RT for Decision Makers in Respiratory Care, vol. 20, no. 1, pp. 20-22, 2007.