Download
1 / 63
630 likes | 921 Views
Ventilation, Transport of gases and oxygen delivery. Dr. Megha Jain. University College of Medical Sciences & GTB Hospital, Delhi. Contents. Lung volumes Mechanics of ventilation Work of breathing Diffusion of gases Transport of gases and oxygen delivery. Lung volumes.

E N D
Ventilation, Transport of gases and oxygen delivery Dr. Megha Jain University College of Medical Sciences & GTB Hospital, Delhi
Contents • Lung volumes • Mechanics of ventilation • Work of breathing • Diffusion of gases • Transport of gases and oxygen delivery
Lung volumes • Tidal volume-Volume of air breathed in or out of the lungs, during quiet respiration. Average: 500ml in adult. • Inspiratory reserve volume- Maximal volume of air which can be inspired after normal tidal inspiration. Average: 3000 ml. • Expiratory reserve volume- Maximal volume that can be expired below normal tidal expiration. Average: 1100ml. • Residual volume- Volume of air remaining in lungs after maximal expiration. Average: 1200ml. • Total lung capacity- Volume of air contained in lungs after maximal inspiration. Average: 5800ml.
Lung volumes • Vital capacity- Maximal volume of air that can be exhaled following maximal inspiration. Average: 60-70 ml/kg. • Functional residual capacity- Lung volume at the end of normal exhalation. Average: 2300ml. • Closing capacity- Volume at which the small airways begins to close in the dependent parts of the lung. Normally – well below FRC, but ↑ with age. It equals FRC in supine position( at around 44 yrs) in upright position( at around 66 yrs) Unlike FRC unaffected by posture.
Ventilation • Defined as mechanical movement of air into and out of the lungs. • Primary mechanism for excretion of Carbon dioxide • Cyclic activity- 2 components • Inward flow of air- Inhalation- active process • Outward flow of air- Exhalation- passive process • Minute ventilation- sum of all exhaled gas volumes in one minute. MV= RR X TV. Normal range= 5 to 10 lts/min in resting state. MV= RR X TV
Ventilation • Dead space ventilation- some of the minute volume occupies space in conducting zones, does not participate in gas exchange and forms anatomic dead space Average in upright position – 150 ml or 2 ml/kg Alveolar dead space- adequately ventilated alveoli not participating in gas exchange as perfusion is absent. Physiologic dead space- sum of anatomic and alveolar dead space. • Alveolar ventilation- volume of inspired gas actually taking part in gas exchange in one minute. AV= RR X (TV – DV) = 12 X (500-150) = 4200 ml/min
Ventilation • Dead space to tidal volume ratio: a numeric index of the total amount of wasted ventilation Vd/Vt = PAco2 – PEco2/PAco2 (N value=0.2 - 0.4) • It represents the primary clinical measure of efficiency of ventilation • Clinical significance: Alveolar ventilation depends on relationship b/w RR and TV. * High RR and low TV result in higher prop. of wasted ventilation per min. * Most efficient breathing pattern is slow and deep breathing.
Effectiveness of ventilation • Ventilation is effective when the body’s need for removal of CO2 is adeqately met. • Under resting metabolic conditions the body produces about 200 ml CO2 per min. • The relative balance b/w CO2 production and alveolar ventilation determines the level of CO2 in lungs and in the blood. PAco2 = V CO2/V A or total CO2 production/CO2 elimination • Normal- alveolar and arterial partial pressures of CO2 are in close equilibrium at approx 40 mmhg.
Effectiveness of ventilation • In cases where alveolar ventilation is ↓ed: rate of CO2 production > rate of excretion thus PA CO2 will rise above its normal value. • Thus, ventilation that is insufficient to meet metabolic needs – hypoventilation • Very high arterial PaCO2 – depress ventilatory response (CO2 narcosis) • Alveolar hypoventilation: by definition it exists when arterial PaCO2 ↑ses above normal range of 37 to 43 mmhg(hypercarbia)
Mechanics of ventilation Forces opposing lung inflation ELASTIC Lung, thorax, surface tension FRICTIONAL Airflow Tissue movement
In intact thorax, Lungs & thorax recoil in opposite directions • Point at which these forces balance = resting vol of lung • AT THIS POINT Ppulm =Patm No air flows Vol. retained in lungs = FRC= 40% of TLC
Elastance Physical tendency to return to original state after deformation Lung vol at any given P is slightly more during deflation than it is during inflation. ↓ HYSTERESIS ↓ (Due to surface tension)
GRAVITY DEPENDENT ventilation exploited to direct ventilation towards healthy lung by changing position of patient
Frictional forces opposing inflation Tissue viscous resistance(20%) Due to tissue displacement during ventilation (lungs, thorax, diaphragm) ↑ by obesity, fibrosis, ascites Airway resistance(80%) Raw = ∆P(driving P)/ ∆V(flow rate) = transrespiratory P/flow rate = 0.5-2.5 cmH2O/L/sec Flow measured by PNEUMOTACHOMETER P measured by PLETHYSMOGRAPH Affected by pattern of flow
Distribution of airway resistance 80% Nose, mouth, large airways TURBULENT FLOW 20% Airways < 2 mm diameter LAMINAR FLOW Branching of airway ↑ total cross sectional area with each generation ↑ area → ↓ velocity→ + laminar flow Deflation - ↑ airway diameter → ↑ resistance Wheezing heard during EXPIRATION
Types of airflow LAMINAR TRANSITIONAL TURBULENT Governed by Poiseulle’s Hagon equation
LAMINAR ∆P = 8ηL X flow π r4 TURBULENT ∆P = flow2 X ρ r5 ↑ Reynold’s number Re = ρ D V η η – viscosity L – length of tube r – radius ∆P – driving P ρ -density 1. Helium is less densebut more viscousthan air Advantageous in turbulent flow but not laminar flow
Inferences from poiseulle’s hagen equation • ∆P = 8ηL X flow π r4 • ∆P αflow r4 • Flow α ∆P X r4 Reducing tube diameter by half requires 16 fold ↑in P to maintain same flow Small changes inbronchial calibercan markedly change flow rates. Basis for - 1. bronchodilator therapy 2. using largest practical size of artificial airway
Flow – volume loops To diagnose lung pathologies as Extra / intrathoracic Variable / fixed Obstructive / restrictive
FIXED AIRWAY OBSTRUCTION VARIABLE Circumferential narrowing Not affected by thoracic P INTRATHORACIC Below 6th tracheal ring Expiratory curve plateaus EXTRATHORACIC Above suprasternal notch Inspiratory curve plateaus
Fixed Variable extrathoracic Variable intrathoracic
Work of breathing • Done by respiratory msls to overcome elastic & frictional forces opposing inflation. W = F X S ( force X distance) = ∆P X ∆V = area under P-V curve Normal breathing – active inhalation - passive exhalation( work of exhalation recovered from potential energy stored in expanded lungs & thorax during inspiration)
Area 1 = work done against elastic forces ( compliance) = 2/3 Area 2 = work done against frictional forces ( resistance work) = 1/3 Area 1+2 = total work done = 2/3 + 1/3 = 1
↑TV → ↑ elastic component of work ↑ RR ( flow) → ↑ frictional work People with diseased lungs assume a ventilatory pattern optimum for minimum work of breathing. COAD Obstructive disease Slow breathing with pursed lips (↓ frictional work) FIBROSIS Restrictive disease Rapid shallow breathing (↓elastic work)
Transport of gases • Diffusion: gas movement b/w the lungs and tissue occurs via simple diffusion. • For O2 there is a stepwise downward cascade of “partial” pressure. PP of oxygen Atmospheric = 147 Alveolar = 100 Arterial = 97 Venous = 40 Tissue = 5
Mechanism of diffusion • Physical process whereby gas molecules move from area of high partial pressure to low one. • Five barriers * RBC * Capillary membrane * Interstitial fluid * Alveolar membrane * Surfactant
Fick’s law of diffusion • Describes bulk movement of gases through biological membranes Vgas = A X D X (P1 – P2)/T A = Cross sectional area D = Diffusion coefficient of gases T = Thickness of memb. P1 – P2 = Diff. in partial pressure • Pulmonary end capillary O2 tension (Pc’O2) depends on: # rate of O2 diffusion # pulmonary capillary blood volume # transit time
Capillary transit time = pulm cap bld vol/CO = 70 ml/5000 ml per min = 0.8 seconds. • High fever, septic shock often cause ↑ed CO, limit diffusion time due to ↑ed blood flow • Maximum Pc’O2 attained after only 0.3 sec ,providing a large safety margin (like exercise where transit time ↓ due to ↑ blood flow) • For practical purposes, Pc’O2 is considered identical to PAO2.
Diffusion capacity • Defined as no. of ml of a specific gas that diffuses across the ACM into the bloodstream each min for each mmhg diff in pressure gradient DLO2 = O2 uptake/ PAO2 - Pc’O2 • Carbon monoxide is preferred over O2 as test gas since its higher affinity for Hb keeps its cap pp very low, so Pc’O2 can be considered as zero DL CO = CO uptake/PA CO • Reduction in DL CO implies impaired gas transfer seen in * abnormal V/Q ratio * destruction of memb * very short capillary transit time
Determinants of alveolar gas tensions • Alveolar O2 tension: * pp of O2 in air (Pi O2 = PB x Fi O2) = 760x0.21 = 159.6 mmhg * accounting for humidification for inspired gases Pi O2 = PB – PH2O x Fi O2 = 760 - 47X0.21 = 149 mmhg * accounting for residual CO2 from previous breaths final alveolar O2 tension is defined by: alveolar air equan: PAO2 = Fi O2 x (PB – 47) – (PA CO2/0.8) = 0.21 x (760 – 47) – (40/0.8) = 99 mmhg. • Arterial O2 tension: approximated by PaO2 = 102 – age/3, n range = 60 – 100 mmhg
Determinants of alveolar gas tensions • Alveolar CO2 tension: PA CO2 = V CO2 x 0.863/V A = 40 mmhg • Arterial CO2 tension: readily measured, n = 38+/-4 mmhg • End tidal CO2 tension: used clinically as an estimate of PaCO2. PA CO2 – PETCO2 gradient is normally < 5 mmhg.
Compliance • Compliance = Distensibility of lung • Elastance = resisting deformation • Compliance = 1/ elastance = ∆V/ ∆P = 0.2L/cm H2O (lung) = 0.2L/cm H2O (Thorax) = 0.1L/cm H2O (lung+ thorax) Affected by Obesity Kyphoscoliosis Ankylosing spondylitis Fibrosis Emphysema
Steep curve + Lt shift = ↑compliance (loss of elastic tissue) Flat curve + Rt shift = ↓compliance (↑ connective tissue)
Compliance Static compliance: measured when air flow is absent, reflects elastic resistance of lung & chest wall. =Corrected tidal vol./(plateau pressure – PEEP) n value: 40 to 60 ml/cm H2O. Dynamic compliance: measured when air flow is present, reflects airway + elastic resistance, = Corrected tidal vol./(peak airway pressure – PEEP) n value: 30 to 40 ml/cm H2O. LOW Compliace: Lung expansion difficult. HIGH Compliance: Incomplete CO2 elimination.
Compliance is reduced in DYNAMIC STATIC Atelectasis ARDS Tension Pneumothorax Obesity Retained secretions Bronchospasm Kinking of ET tube Airway obstruction
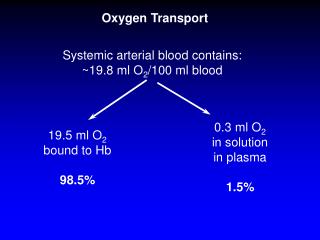
Transport of oxygen • 2 forms: 1. Small amount dissolved in plasma 2. Chemically combined with Hb in RBC • Dissolved oxygen: henry’s law Gas conc = S x PP in soln * S - gas solubility coefficient for given soln at a given temp Dissolved O2 = 0.003 x 100 = 0.3ml/dl
Transport of oxygen • Chemically combined with Hb: accounts for max blood oxygen • Hemoglobin - conjugated protein: four polypeptide (globin) chain, each combined with a porphyrin complex called heme. • each heme complex has a central ferrous ion to which O2 binds converting Hb into oxygenated state. • 1 gram of normal Hb carries 1.34 ml of O2, if Hb is 15 g/dl , O2 carrying capacity of blood = 1.34 ml x 15 g/dl = 20.1 ml/dl
Transport of oxygen • O2 content: dissolved + combined with Hb • O2 content = (0.003 x PO2) + (Hb x 1.34 x SaO2) = (0.003 x 100) + (15 x 1.34 x 0.975) = 19.5 ml/dl (arterial) • O2 content = (0.003 x 40) + (15 x 1.31 x 0.75) = 14.8 ml/dl (venous)
Transport of oxygen • Total oxygen delivery to tissues: = oxygen content x CO = 20 ml/dl x 50 dl blood/min = 1000 ml/min. • O2 Flux: amount of O2 leaving the left ventricle per min in the arterial blood. • Fick equation describes O2 consumption (VO2) = CO x diff b/w arterial and venous oxygen content = 250 ml/min. • Extraction ratio for O2= (Ca O2 - Cv O2)/ Ca O2 = 5/20 = 25%
Oxygen stores • Normally in adults = 1500 ml * O2 remaining in lungs * bound to Hb * dissolved in body fluids • O2 contained within lungs at FRC – most imp source of oxygen. • Apnea in pt breathing room air = FiO2 x FRC = 0.21 x 2300 = 480 ml depleted in 90 sec • Preoxygenation with 100% oxygen for 4-5 min leaves 2300 ml of oxygen – delays hypoxemia following apnea
HbO2 Dissociation Curve • Relates SpO2 to the PO2 • Sigmoid shaped (comb of 1st heme Hb molecule with O2↑ affinity of other heme molecules) SHIFTING AFFINITY
Measure of Hb affinity for O2 • quantified by P50. • P50 - PO2 at which Hb is 50% saturted. • P50 = 26 mmhg at PCO2 40 mmhg, pH 7.4, temp. 37°C. ↑ P50 (facilitates O2 release) ↓ Hb affinity, Rt shift of ODC
Factors affecting O2 loading and unloading • Blood pH • Body temp • Organic phosphates in RBC • Variations in structure of Hb
Shift of curve to right • Fall in blood pH due to a. ↑ CO2 b. Presence of any acid in blood • ↑ temp • Inhalational anesthetics: Isoflurane shifts P50 to right by 2.6 mmhg. • ↑ conc of 2,3- DPG • By product of glycolysis (accumulates in anaerobic met.) • Competes with O2 for binding sites on Hb • ↓ in: acidosis, blood stored in acid citrate dextrose sol in blood bank • ↑ in: high altitude, chronic anemia, exercise