Download
1 / 1
20 likes | 211 Views
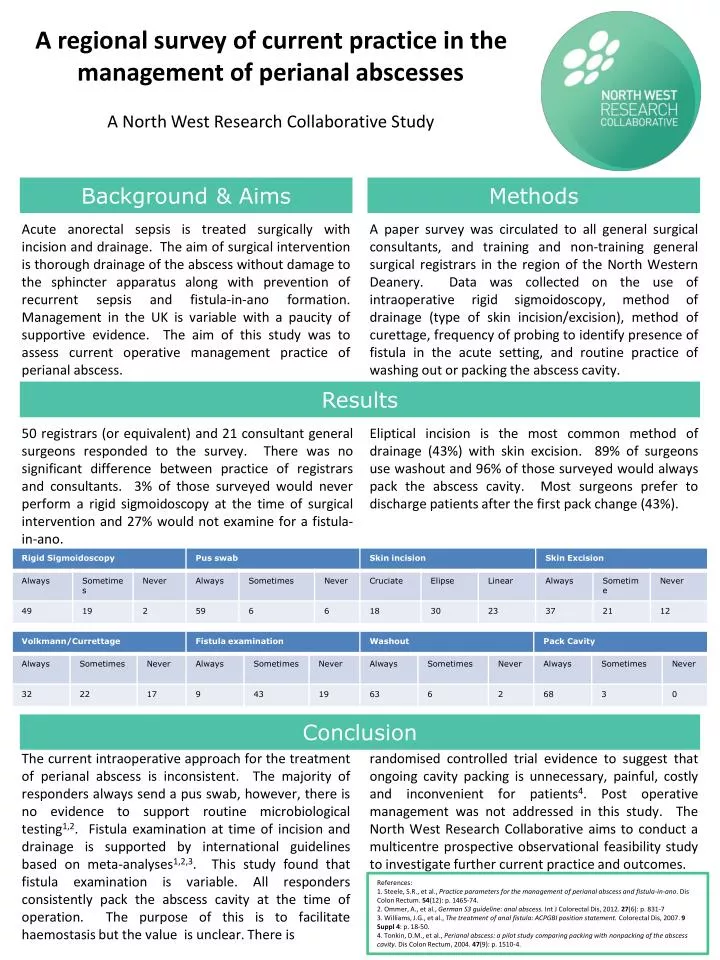
A regional survey of current practice in the management of perianal abscesses A North West Research Collaborative Study. Background & Aims. Methods.

E N D
A regional survey of current practice in the management of perianal abscesses A North West Research Collaborative Study Background & Aims Methods Acute anorectal sepsis is treated surgically with incision and drainage. The aim of surgical intervention is thorough drainage of the abscess without damage to the sphincter apparatus along with prevention of recurrent sepsis and fistula-in-ano formation. Management in the UK is variable with a paucity of supportive evidence. The aim of this study was to assess current operative management practice of perianal abscess. A paper survey was circulated to all general surgical consultants, and training and non-training general surgical registrars in the region of the North Western Deanery. Data was collected on the use of intraoperative rigid sigmoidoscopy, method of drainage (type of skin incision/excision), method of curettage, frequency of probing to identify presence of fistula in the acute setting, and routine practice of washing out or packing the abscess cavity. Results 50 registrars (or equivalent) and 21 consultant general surgeons responded to the survey. There was no significant difference between practice of registrars and consultants. 3% of those surveyed would never perform a rigid sigmoidoscopy at the time of surgical intervention and 27% would not examine for a fistula-in-ano. Eliptical incision is the most common method of drainage (43%) with skin excision. 89% of surgeons use washout and 96% of those surveyed would always pack the abscess cavity. Most surgeons prefer to discharge patients after the first pack change (43%). Conclusion The current intraoperative approach for the treatment of perianal abscess is inconsistent. The majority of responders always send a pus swab, however, there is no evidence to support routine microbiological testing1,2. Fistula examination at time of incision and drainage is supported by international guidelines based on meta-analyses1,2,3. This study found that fistula examination is variable. All responders consistently pack the abscess cavity at the time of operation. The purpose of this is to facilitate haemostasis but the value is unclear. There is randomised controlled trial evidence to suggest that ongoing cavity packing is unnecessary, painful, costly and inconvenient for patients4. Post operative management was not addressed in this study. The North West Research Collaborative aims to conduct a multicentre prospective observational feasibility study to investigate further current practice and outcomes. References: 1. Steele, S.R., et al., Practice parameters for the management of perianal abscess and fistula-in-ano.Dis Colon Rectum. 54(12): p. 1465-74. 2. Ommer, A., et al., German S3 guideline: anal abscess.Int J Colorectal Dis, 2012. 27(6): p. 831-7 3. Williams, J.G., et al., The treatment of anal fistula: ACPGBI position statement. Colorectal Dis, 2007. 9 Suppl 4: p. 18-50. 4. Tonkin, D.M., et al., Perianal abscess: a pilot study comparing packing with nonpacking of the abscess cavity.Dis Colon Rectum, 2004. 47(9): p. 1510-4.