Download
1 / 37
370 likes | 628 Views
Skin infection and infestation. Philip G. Murphy Consultant Microbiologist, AMNCH, Tallaght Clinical Professor, TCD Tel ext : 3919 email : philip.murphy@amnch.ie. Lecture objectives. Skin microbiology Common skin infections Emergency skin infections Less common infections

E N D
Skin infection and infestation Philip G. Murphy Consultant Microbiologist, AMNCH, Tallaght Clinical Professor, TCD Tel ext : 3919 email : philip.murphy@amnch.ie
Lecture objectives • Skin microbiology • Common skin infections • Emergency skin infections • Less common infections • Non-bacterial infections
Normal skin flora • Resident: Coag. Neg. Staph, micrococci, diphtheroids anaerobes eg propionibacteria • Transient: environmental contamination Staph. aureus, gram negatives survive a few hours, reduced by washing and skin antibacterial substances Staph aureus carriage: nose - 10-30 % outside hospital 20-60 % in hospital staff
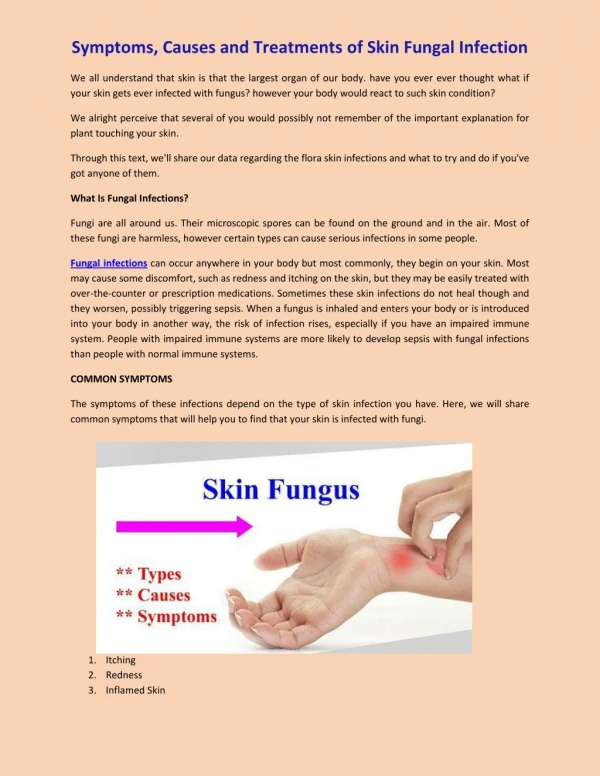
Pathogens 1 • Staphylococcus aureus • Streptococcus pyogenes (Group A Strep) • Other haemolytic Strep • Anaerobes: Clostridia, cocci • Other bacteria: Corynebacterium diphtheriae, C. minutissimum, Erysipelothrix rhusiopathiae, Mycobacteria, Pseudomonas, Treponema, B. burgdorferi • Viruses: HS, VZ, Molluscum, Papovavirus, Coxsackie • Fungi: C. albicans, Microsporum, Trichophyton, Epidermophyton floccosum
Pathogens 2 • Protozoa: Leishmania in Africa, Asia S. America • Helminths: Onchocerciasis, Loa Loa, Strongyloides • Arthropod: Sarcoptes scabiei, Pediculosis (lice)
Skin ulcers • vascular ulcers: skin flora No Rx If pathogens +/- Rx • Pseudomonas aeruginosa - ecthyma gangrenosum • Anaerobes - Meleneys & Fournier’s gangrene • Treponema - chancre • M.tuberculosis - lupus vulgaris • M. ulcerans - Buruli ulcer • Borrelia vincenti - tropical ulcer
Furuncles (Boils) and Carbuncles • Boils (furuncles) Staph. aureus lesions in hair follicles or sebaceous glands • Carbuncles are larger deeper involving >1 hair follicle eg back of neck • If recurrent check blood glucose. • Rx flucloxacillin +/- Fusidic acid etc. +/- drainage
Cellulitis and Erysipelas • Spreading erythema and swelling Erysipelas when intradermal and due to GpAStrep • 90% Haemolytic Strep (Group A) • 10% Staphylococcus aureus • ? Anaerobe involvement Rx: Penicillin + Flucloxacillin Clindamycin + Ciprofloxacin
Folliculitis • Infection of hair follicles • usually pustular folliculitis • Clinical presentation • follicle-centred pustules • e.g. in scalp, groin, beard & moustache (sycosis barbae) • Mostly (95%) due to Staphylococcus aureus • Treatment: oral flucloxacillin
Impetigo Crusted vesicles on face/arms in children Group A Strep. (Strep. pyogenes) • +/- Staphylococcus aureus 2o infection • infectious • Impetigo neonatorum = Bullous impetigo due to Staphylococcus aureus (Group II, PT 71) Rx: isolation, skin disinfection, antibiotic if severe
Gas Gangrene • Myonecrosis, gas production, sepsis • Rapid onset and toxaemia / shock • Crepitus, brawny oedema • Foul-smelling discharge, brown skin discoloration, bullae, • May advance 1“ per hour! • Disproportionate pain. • Mortality > 25% Microbiological emergency Caused by exotoxin-producing Clostridium perfringens usually after direct inoculation of contaminated, ischaemic wound
Necrotising Fasciitis Fig 1 Young woman presenting with cellulitis of her lower abdomen after a caesarean section five days earlier. Small areas of skin necrosis are clearly visible Fig 2 Late signs of necrotising fasciitis with extensive cellulitis, induration, skin necrosis, and formation of haemorrhagic bullae Rx Surgery + Penicillin & Clindamycin
Gangenous cellulitis • Necrotising fasciitis • Type I polymicrobial (GNB, AnO2) • Type II Gp A Strep • Gas gangrene, (Clostridium perfringens) • Progressive synergistic gangrene (post op) • Synergistic necrotising • Immune compromised (Pseudomonas)
Ritter’s DiseaseorToxic epidermal necrolysis, or Lyell’s Syndrome or scalded child syndrome • Toxaemia, fever, • erythematous, tender skin lesions • Staph aureus Group II PT71 • toxin induced split epidermis Rx: Isolation, Skin disinfection, flucloxacillin
Toxic Shock Syndrome • Fever, rash, hypotension, GIT signs, myalgia, confusion, desquamation • genital or non genital • TSST-1 or enterotoxin • 30% recurrence with low TSST-1 Ab • Flucloxacillin, Ig.
Pyoderma • Skin lesions due to Strep. pyogenes /Staph. aureus • Scrum pox, scabies, eczema, herpes • nephritogenic strains (M types 49, 55) • Gangrene • Rx: debridement + antibiotics (necrotizing fasciitis Fournier/Meleneys)
Lyme DiseaseBorrellia burgdorferi Erythema chronicum margans Rx amoxycillin, 3rd gen cephalosporins
Abscesses • Subcutaneous: axillae, groin, perineum postpartum breast • If foreign body - must remove • usually Staph. aureus, less commonly Strep. pyogenes • Also anaerobes, TB, • Rx: Drainage +/- antibiotic
Paronychia • Infection of subcutaneous tissue around nailbed • Staph aureus, Strep pyogenes, Herpes simplex • Chronic form with loss of cuticle due to wet hands due to gram negatives, or yeasts
Animal bites • Pasturella multocida Rx: penicillins +/- anaerobes • Others: Tetanus Rabies Cat scratch fever (Bartonella hensellae)
Others • Erysipeloid: Erysipelothrix rhusiopathiae blue-red discolouration with a sharp edge Rx: pen • Erythrasma: Corynebacterium minutissimun Rx: Ery • Acne vulgaris: skin flora ?Rx: Tet • Lyme Disease: Borellia burgdorferi Rx: amp/cefotax. • Diphtheria, burns, Anthrax, Leprosy, Yaws, Pinta Erythema chronicum margins in Lyme Disease
Other viral • Warts: Papovavirus • Molluscum contagiosum: Pox virus • Orf, Milker’s Nodule: Pox viruses • Fifth Disease: Parvovirus Varicella zoster(chickenpox) Measles Erythyma infectiosum (Fifth Disease or slapped cheek syndrome) Molluscum contagiosum
Fungal • Tinea (ringworm): Trichophyton, Microsporum, Epidermophyton Tinea capitis (scalp ringworm) M. audouini, T. schoenleinii Tinea corporis (body ringworm) Trichophyton spp. Tinea pedis (athlete’s foot) T rubrum,T. mentagrophytes var. interdigitalis, E. floccosum Tinea barbae (beard ringworm) T. verrucosum Tinea cruris (groin ringworm) T. rubrum, E. floccusum Tinea unguium (Nail ringworm) T. rubrum Rx: antigungals: eg. terbinafine, griseofulvin • Pityriasis versicolor: Malassezia furfur • Sporotrichosis: Sporotrichium schenckii • Mycetoma: Actinomyces,Streptomyces, Nocardia Tinea corporis
Tinea pedis - usually between toes Dermatophyte infection: Trychophyton rubra, T. mentagrophytes, T. floccusum
Infestations • Scabies: Sarcoptes scabiei mite Norwegian crusted • Fleas: Pulex irritans (human flea) Xenpopsylla cheopsis (Rat flea : Plague) • Lice: Pediculosis Pediculus capitis (head louse) Pediculus corporis (body louse) Pythirus pubis (pubic or crab louse) May transmit Typhus (Rickettsia prowazeki) Relapsing fever (Borellia recurrentis) Rx: 1/2% Malathion topically
Candida nail infection Nappy rash Candida albicans not amoniacal
Roseola infantum viral, incubation 10-15 d follows sore throat and fever - mistaken for pen allergy
Leishmania tropica dog, sandfly hosts
Kawaski disease ? Infectious platelates raised, desquamation coronary artery aneurysms
“ampicillin rash” seen in 2/3 rd’s of patients with infectious mononucleosis on ampicillin for “sore throat”
Ecthyma: exudate or crust of a pyogenic infection involving the entire epidermis. Usually the consequence of neglected impetigo caused by Staphylococcus aureus or group A streptococcus. Can evolve from localized skin abscesses (boils) or within sites of preexisting trauma. The margin of the ecthyma ulcer can be indurated, raised, and violaceous. Untreated ecthymatous lesions can enlarge over the course of weeks or months to a diameter of 2 to 3 cm. Staphylococcal and streptococcal ecthyma occur most commonly on the lower extremities of children, the elderly, and people who have diabetes. Poor hygiene and neglect are key elements in its pathogenesis. Ecthyma gangrenosum: single or multiple, cutaneous or mucous membrane ulcers that are most often associated with prolonged neutropenia, Pseudomonas aeruginosa bacteremia, and other serious bacterial infections. It resembles ecthyma caused by staphylococcal or streptococcal organisms. First presenting as a painless nodular lesion, it quickly develops a central hemorrhagic area that subsequently breaks down to form a large necrotic ulcer.
Factitious Ulcer Self induced Young adults HCW or associated with No distress Easy reach of dominant hand Personality: infantile,dependent,manipulative Film “The Secretary”
Erysipelothrix rhusiopathiae Orf / Molluscum contagiosum Anthrax Sarcoptes scabei Leprosy Chancroid : Haemophilus ducreyii Lymphogranuloma venereum: Chlamydia Bedbug (cimex leticularis)