Download
1 / 11
230 likes | 1.87k Views
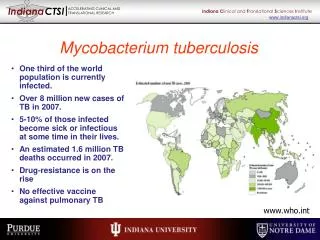
Mycobacterium tuberculosis -Characteristics. Gram positive Obligate aerobe Non-spore-forming Non-motile rod Mesophile 0.2 to 0.6 x 2-4um 1 Slow generation time: 15-20 hours May contribute to virulence 1 Lipid rich cell wall contains mycolic acid—50% of cell wall dry weight 1

E N D
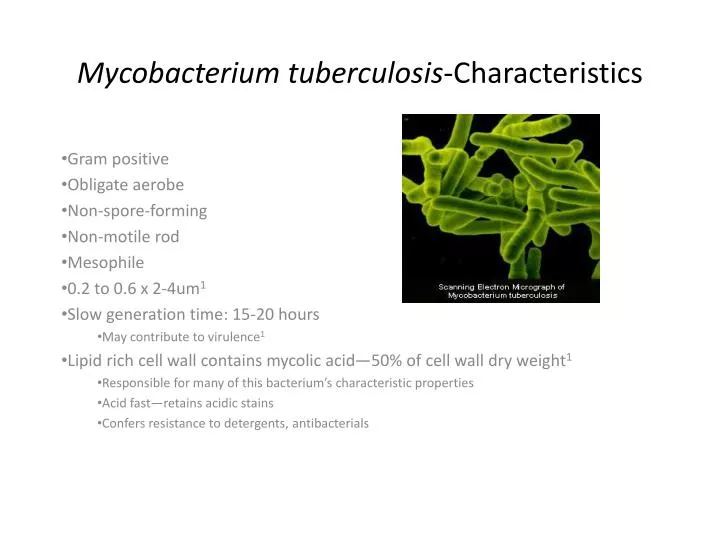
Mycobacterium tuberculosis-Characteristics Gram positive Obligate aerobe Non-spore-forming Non-motile rod Mesophile 0.2 to 0.6 x 2-4um1 Slow generation time: 15-20 hours May contribute to virulence1 Lipid rich cell wall contains mycolic acid—50% of cell wall dry weight1 Responsible for many of this bacterium’s characteristic properties Acid fast—retains acidic stains Confers resistance to detergents, antibacterials
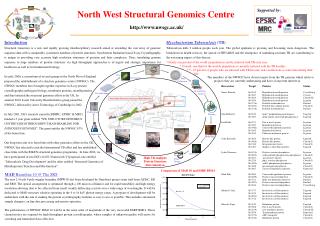
Diagnostics of Mycobacterium • Initial screening: • TB skin test (Purified Protein Derivative). • Drawbacks: BCG injected subjects are positive, 3 days delay for result • QFT-G test (measures INF- response to TB specific antigen) • TB tests Active, depending on the suspected location of bacterium: • 3-5 samples of sputum • multiple gastric aspirate • urine (UTI) • CSF (meningeal)2 • Cultures • Samples are processed for fast acid stain (FAS smear positive indicates Mycobacterium) and cultured after alkali decontamination (30s in 1-2% NaOH) • Molecular methods use species-specific genes, including light and heave ribosomal RNA3 Clinical specimen/ decontamination culture • Direct detection: • Microscopy • PCR • MTB rifampin resistance • Species identification: • 16S rRNA hybridization (MTB and MAC) • 16S rRNA gene PCR sequencing (NTM) • restriction fragment length polymorphism Susceptibility testing Rifampin resistance (PCR oligohybridization sequencing)
M. Tuberculosis mechanisms • Facultative intracellular pathogen • Does not produce toxin • Manipulates phagocytosis -uses phagocytic vacuole for survival and replication -uses multiple ligand-receptor interactions to promote phagocytosis - prevents fusion of phagosome with lysosome5
Benefits of Phagocytosis • Protection from expulsion • Less hostile environment with supplied nuturients • Allows for mobility5
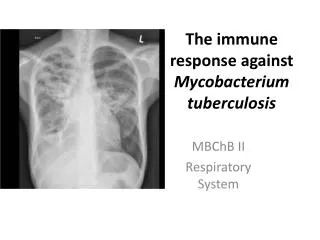
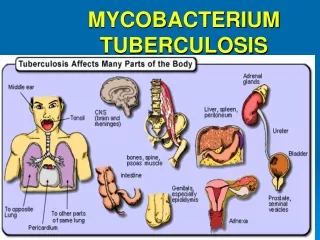
Inactive disease- “latent” stage Active Disease --pulmonary tuberculosis -extrapulmonary tuberculosis -disseminated tuberculosis -lymph node tuberculosis -pleural tuberculosis -genitourinary tuberculosis -skeletal tuberculosis -central nervous system tuberculosis -abdominal tuberculosis -pericardial tuberculosis6 Pathogen Targets
Symptoms • What are the symptoms of TB? • Fever • Fatigue • Weakness • Weight loss • Night sweats • Symptoms of pulmonary TB include: • Coughing • Pleurisy (pain when taking deep breaths) • Coughing up blood4.
How is TB treated? Optimal treatment of TB utilizes a combination of 2 to 3 antibiotics taken over a period of 6 to 9 months. Drug resistant strains of TB are not uncommon, which is why multiple antibiotics are used together during treatment. Drugs used most commonly to treat TB include isoniazid, rifampin, ethambutol, and pyrazinamide7.
What are some complications that can occur from TB infection? Untreated TB infections can cause severe damage in the infected organ, miliary TB develop which is TB that has spread throughout the entire body, and death. It is important that patients adhere to their medication during the full duration of their treatment, otherwise drug resistance can develop8.
Is there a vaccine for this TB? BCG (Bacille Calmette-Guerin) vaccine is an attenuated vaccine that is used in many countries around the world where TB prevalence is high. In the U.S. however, the vaccine is not generally recommended because of the low risk of infection, its variable effectiveness, and its interference with TB skin test reactivity9.
Drug sensitivity The raise of drug-resistance strains makes strain identification necessary for the selection of the proper pharmacological treatment. Several genes have been found to confer specific drug-resistances. Such genes are now readily identified using molecular techniques (most of them PCR-amplification based), at least for the already sequenced drug-resistance associated genes. Identification and characterization of unknown types of resistance requires de-novo studies3. Genetic targets relevant for direct detection of antimycobacterial drug resistance development
References 1. Todar, K. (2009). Mycobacterium tuberculosis and Tuberculosis. Retrieved November 2, 2009 from Online Textbook of Bacteriology website: http://www.textbookofbacteriology.net/ tuberculosis.html. 2. Centers for Disease Control and Prevention, American Association for Clinical Chemistry, ed. board R.B. Carey, PhD, Chief, Epidemiology and Laboratory Branch, published Sept. 29, 2008, last modified on November 6, 2009: http://www.labtestsonline.org/understanding/conditions/tuberculosis-3.html 3. S.V. Balasingham, T. Davidsen, I. Szpinda, S.A. Frye, T. Tønjum. Molecular diagnostics in tuberculosis: basis and implications for therapy. Mol Diagn Ther. (2009); vol. 13: p. 137-51. doi: 10.2165/01250444-200913030-00001. Review 4. County of Orange, CA Health Care Agency. Tuberculosis Treatment and Services. Retrieved November 6, 2009 from http://www.ochealthinfo.com/docs/public/tb/tb-brochure.pdf. 5. Ernst, JD, Stendahl, O (2006). Mycobacterium tuberculosis: mechanisms of phagocytosis and intracellular survival. In Henderson, B, Wilson, M, Coates A, Curtis, M (Eds.), Phagocygtosis of Bacteria and Bacterial Pathogenicity (chp. 8, pp. 246-265). Cambridge: Cambridge University Press. 6. Cole, ST (2005). Overview of clinical tuberculosis. In Cole, ST, Eisenach, KD, McMurray, DN, Jacobs, WR (Eds.), Tuberculosis and the tubercle Bacillus (chp. 2, pp. 17-29). Washington: ASM Press. 7. "Tuberculosis." American Lung Association. ALA, 1 Jan. 2004. Web. 20 Oct. 2009. <www.lungusa.org/lung-disease/tuberculosis.htm>. 8. "Tuberculosis." Global Tuberculosis Institute. New Jersey Medical School, 1 May 2009. Web. 20 Oct. 2009. <www.umdnj.edu/ntbcseb/diagnosis.htm>. 9. "BCG Vaccine." CDC.com. Centers for Disease Control, 1 June 2009. Web. 20 Oct. 2009. <www.cdc.gov/tb/publications/factsheets/prevention/BCG.htm>.