Download
1 / 20
250 likes | 646 Views
Brugada Syndrome. Morning Report June, 2008 Jessie Stewart. Why Present Brugada?. 1. Lots of us missed it. 2. A new discovery- first described in 1992. 3. Drs. Josep, Pedro and Ramon Brugada. Where are we going?. Primary Goal Understanding Brugada Prevalence Presentation Prognosis

E N D
Brugada Syndrome Morning Report June, 2008 Jessie Stewart
Why Present Brugada? 1. Lots of us missed it. 2. A new discovery- first described in 1992. 3. Drs. Josep, Pedro and Ramon Brugada.
Where are we going? • Primary Goal • Understanding Brugada • Prevalence • Presentation • Prognosis • Therapy
Goal Recognize Brugada I: coved ST segment in V1-V3, >2mm elevation, inverted T wave.
Brugada Syndrome is… • A sodium channel abnormality that predisposes to sudden cardiac death. • Characterized by specific EKG patterns: • Type I is diagnostic when combined with the right clinical picture. • Types II and III raise suspicion for Brugada but they are only diagnositic if they can be converted to Type I during challenge with a sodium channel blocker. • These patterns are dynamic and inducible.
Type I- Diagnostic • V1-V3 (as least two leads) ST segment elevation >2mm, “coved” shape, inverted T-wave. • Coupled with • Documented VFib • Polymorphic VT • FH of sudden cardiac death <45 yo • Type I EKG in family members • VT inducable in EP lab • Syncope • Nocturnal agonal respiration
Types II and III- Suggestive • II: V1-V3 ST segment elevation >2mm, “saddleback” shape, pos or biphasic T. • III: <1 mm elevation, either coved or saddleback.
SCN5A gene • Codes for cardiac sodium channel that opens during phase 2 of the action potential. In Brugada, it opens poorly in RV epicardial cells. • Autosomal dominant inheritance • 20-30% of cases have anbl SCN5A gene. • 80+ mutations, differing prognosis. 1 0mVolts 2 0 3 1 -85mVolts 4 4 4 Priori, S. G. et al. Circulation 1999;99:674-681
Defective sodium channels: shorter AP (phase 0), deeper notch (phase I), and shorter phase 2. Creates juxtaposition of depolarized and repolarized cells, setting up possibility of PHASE 2 RENTRY, closely grouped PVCs, and VT or V Fib. On EKG, ST segment not at baseline because no longer have uniform depolarization of the entire ventricle. Nattel and Carlsson Nature Reviews Drug Discovery5, 1034–1049 (December 2006) | doi:10.1038/nrd2112
Where are we going? • Primary Goal • Understanding Brugada • Prevalence • Presentation • Prognosis • Therapy
Prevalence • In Thailand, estimated to be the second leading cause of death in men <40, after accidents. • In the Philippines, known as Bangungut- scream followed by sudden death during sleep- and in Japan as Pokkuri- unexpected sudden death at night. • At the Carolinas Medical Center, Charlotte, found in 0.4% of all EKGs.
Presentation • Sudden cardiac arrest often the first symptom. • More common at night, esp when sleeping. • Ages 22-65- mean age of sudden death 41 +/- 15 years.
Where are we going? • Primary Goal • Understanding Brugada • Prevalence • Presentation • Prognosis • Therapy
Prognosis Risk Stratification based on- 1. Prior History of SCA: 69% recur within 5 years. 2. History of syncope 3. EKG abnormal at baseline or only after drug challenge? 4. Is a SVA inducible in the EP lab? SCA- Sudden Cardiac Arrest SVA- Sustained Ventricular Arrhythmia
Prognosis In 547 patients with type 1 Brugada syndrome with no prior history of SCD, the probability of SCA or VF during follow-up (average 2 years) - Overall 8.2% with SCA or VFib. Adapted from Brugada, J, Brugada, R, Brugada, P, Circulation 2003; 108:3092 SCA- Sudden Cardiac Arrest SVA- Sustained Ventricular Arrhythmia
Where are we going? • Primary Goal • Understanding Brugada • Prevalence • Presentation • Prognosis • Therapy
Treatment • Implantable Cardiac Defibrillator Prior History of SCA: 69% recur within 5 years.
Drug Therapy? • Quinidine (Class IA) may blunt Ito. • Isoproterenol (Beta-adrenergic agonist) may augment L-type Ca++ current.
Goal Recognize Brugada I: coved ST segment in V1-V3, >2mm elevation, inverted T wave.
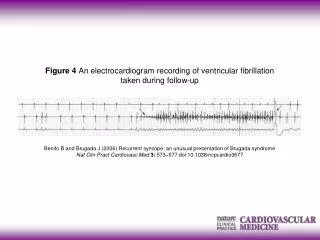
References • Antelevitch C et al. Brugada Syndrome: Report of the Second Consensus Conference. Heart Rhythm 2005. 2(4):429-440. • Benito and Brugada. Recurrent syncope: an unusual presentation of Brugada syndrome. Nature Clinical Practice 2006. 3(10): 573-577. • Brugada, J, Brugada, R, Brugada, P. Determinants of Sudden Cardiac Death in Individuals With the Electrocardiographic Pattern of Brugada Syndrome and No Previous Cardiac Arrest. Circulation 2003; 108:3092. • Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome: a multicenter report. J Am Coll Cardiol. 1992; 20: 1391–1396. • UpToDate. Brugada Syndrome and Sudden Cardiac Arrest. • Priori, S. G. et al. Genetic and Molecular Basis of Cardiac Arrhythmias: Impact on Clinical Management Part III. Circulation 1999;99:674-681.