Download

1 / 55
550 likes | 613 Views
Learn about the symptoms, diagnosis, and treatment of acute pericarditis, including pericardial physiology, chest pain characteristics, pericardial friction rub, cardiac tamponade pathophysiology, common etiologies, and physical findings. Understand the Beck triad and Pulsus Paradoxus.

E N D
AcutePericarditis Yrd.Doç. Dr. Olcay ÖZVEREN
Pericardial physiology includes 3 main functions. • First, through its mechanical function, the pericardium promotes cardiac efficiency by limiting acute dilation, maintaining ventricular compliance with preservation of the Starling curve, and distributing hydrostatic forces. The pericardium also creates a closed chamber with subatmospheric pressure that aids atrial filling and lowers transmural cardiac pressures. • Second, through its membranous function, the pericardium shields the heart by reducing external friction and acting as a barrier against extension of infection and malignancy. • Third, through its ligamentous function, the pericardium anatomically fixes the heart.
Chest pain is the cardinal symptom. • The quality of the pain may be sharp, dull, aching, burning, or pressing. • Intensity varies from barely perceptible to severe. • Pain is usually precordial with referral to the trapezius ridge. • It is worse during inspiration, when lying flat, or during swallowing and with body motion
A pericardial friction rub is pathognomonic for acute pericarditis. • The rub has a scratching, grating sound similar to leather rubbing against leather. • Auscultation with the diaphragm of the stethoscope over the left lower sternal edge allows the best detection of the rub. • Auscultation during end expiration with the patient sitting up and leaning forward increases the likelihood of observing this physical finding. • Serial examinations may be necessary for detection. • More than 50% of rubs are triphasic. They are composed of (1) an atrial systolic rub that precedes S1, (2) a ventricular systolic rub between S1 and S2 and coincident with the peak carotid pulse, and (3) an early diastolic rub after S2 (usually the faintest). • The biphasic to-and-fro rub is less common (24%). It can occur with tachycardia and is due to summation of the atrial and early diastolic rub. • Monophasic rubs (the ventricular systolic) are the least common but may occur in patients with atrial fibrillation. • Especially when it is monophasic, the pericardial friction rub can be mistaken for a systolic murmur. Pericardial rubs may be differentiated if the rub does not change with usual respiratory or positional maneuvers, if 3 components are present, and if the findings on the ECG are typical.
Pathophysiology • 3 phases of hemodynamic changes in tamponade.1 • Phase I: The accumulation of pericardial fluid causes increased stiffness of the ventricle, requiring a higher filling pressure. During this phase, the left and right ventricular filling pressures are higher than the intrapericardial pressure. • Phase II: With further fluid accumulation, the pericardial pressure increases above the ventricular filling pressure, resulting in reduced cardiac output. • Phase III: A further decrease in cardiac output occurs, which is due to equilibration of pericardial and left ventricular (LV) filling pressures.
Rapid accumulation of pericardial fluid may cause elevated intrapericardial pressures with as little as 80 mL of fluid, while slowly progressing effusions can grow to 2 L without symptoms
etiology Infectious • viral. • Pyogenic • Tuberculous • Fungal (histoplasmosis, coccidioidomycosis, Candida) • Other infections (syphilitic, protozoal, parasitic) • Neoplasia • Postoperative/postprocedural • Uremia • Myxedema • Severe pulmonary hypertension • Radiation therapy • Acute myocardial infarction, • Aortic dissection, • Trauma • Familial Mediterranean fever • Systemic lupus erythematosus • Drug-associated (eg, procainamide, hydralazine, isoniazid, minoxidil, phenytoin, anticoagulants, methysergide
Physical findings • TheBecktriadoracutecompressiontriad • Described in 1935, thiscomplex of physicalfindingsrefersto • increasedjugularvenouspressure, • hypotension, • anddiminishedheartsounds.
Normal inspirasyon esnasında sistemik arteryel basınçta 5-8 mmHg’lık düşüş normaldir. • Kalp tamponadında sistolik arter basıncı normal inspirasyonda 10 mmHg veya daha fazla düşer, buna “Pulsus Paradoksus” denir ve tamponad için önemli bir bulgudur. • Pulsus paradoksusun nabız bulgusu olarak algılanabilmesi için ekspiryum-inspiryum arasındaki sistolik basınç farkının 20 mmHg’nın üzerinde olması gerekmektedir. Bu durumlarda hastanın abdomeni izlenir, inspirasyon ile abdomen yükseldiği anda radiyal nabız zayıflar veya kaybolur. • Pulsus paradoksus invaziv arteryel monitörizasyonla veya noninvaziv olarak değerlendirilebilir. Noninvaziv olarak tansiyon aletinin manşonu sistolik kan basıncının 15 mmHg üzerine kadar şişirilir, sonra sistolik seslerin ilk olarak duyulduğu noktaya kadar manşonun havası yavaş yavaş indirilir. Daha sonra tüm atımlar devamlı olarak duyuluncaya kadar indirmeye devam edilir. İlk sistolik seslerin kesintili olarak duyulduğu nokta ile korotkoff seslerin devamlı olarak duyulduğu nokta arasındaki fark pulsus paradoksusun büyüklüğünü verir. • Pulsus paradoksusun nedeni; kalp tamponadında inspirasyonda bir miktar azalan intraperikardiyal basınç, sağ ventrikülün diyastol diyastol başında hızla dolmasına izin verir ve bu doluşla iyice artan sağ ventrikül diyastolik basıncı interventriküler septumu sol ventriküle doğru iter. Septumun sola doğru kaymasıyla küçülen sol ventrikül kavitesinin diyastolik doluşu azalır. Buna inspirasyon sırasında artan pulmoner venöz göllenme eklenir ve sonuçta sol ventrikül atım volümü, dolayısıyla sistolik kan basıncı daha da düşerek pulsus paradoksus meydana gelir.
Kalp tamponadındavenöz dönüşün ve kalp doluşunun engellenmesi boyun ven dolgunluğunun ileri derecede artmasına ve venpulsasyonlarında belirgin değişikliklere neden olur.
Normalde kalbe olan venöz dönüş, boyun venlerinin ventrikül sistolüne rastlayan X çöküntüsü ve atriyumların boşalmalarına rastlayan Y inişi süresince olur. Kalp tamponadında ventrikül volümü hızlı ejeksiyon esnasında hızla küçüldüğü için intraperikardiyal basınç ve sağ atriyum basıncı da hızla düşer ve bunun sonucunda X çöküntüsü belirgin olur. İntraperikardiyal basınç yüksekliği nedeniyle ventrikül diyastolü tam olmadığı ve tüm diyastol boyunca kompresyon olduğu için Y inişi yavaşlar, hatta kaybolur.
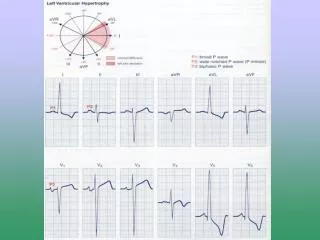
ECG • Elektrokardiyografi (EKG) normal olmakla birlikte sıklıkla nonspesifik değişiklikler özellikle de ST-T dalga değişiklikleri bulunur. • Kalbin perikard sıvısı içerisinde yüzmesine bağlı olarak QRS kompleksinde nadiren de P ve/veya T dalgasını da kapsayacak şekilde üç veya dört atımda bir voltaj değişikliği izlenir ve bu durum “elektriki alternans” olarak adlandırılır. • Hem P hem de QRS komplekslerinde elektriki alternans izlenmesi tamponad için spesifiktir. • QRS voltajında azalma izlenir.
ekokardiyografi Pericardial efusion Early diastolic collapse of the right ventricular free wall Late diastolic compression/collapse of the right atrium Ivc pleathore Swinging heart A greater than 40% relative inspiratory augmentation of right-side flow A greater than 25% relative decrease in inspiratory flow across the mitral valve
management • All patients should receive the following: • Oxygen • Volume expansion with blood, plasma, dextran, or isotonic sodium chloride solution, as necessary to maintain adequate intravascular volume: Sagrista-Saauleda et al noted significant increase in cardiac output after volume expansion.14 • Bed rest with leg elevation: This may help increase venous return. • Inotropic drugs (eg, dobutamine): These can be useful because they do not increase systemic vascular resistance while increasing cardiac output
Positive-pressure mechanical ventilation should be avoided because it may decrease venous return and aggravate signs and symptoms of tamponade
pericardiocentesis • Removal of pericardial fluid is the definitive therapy for tamponade and can be done by the following 3 methods. • Emergency subxiphoid percutaneous drainage: This is a life-saving bedside procedure. The subxiphoid approach is extrapleural; hence, it is the safest for blind pericardiocentesis. A 16- or 18-gauge needle is inserted at an angle of 30-45° to the skin, near the left xiphocostal angle, aiming towards the left shoulder. When performed emergently, this procedure is associated with a reported mortality rate of approximately 4% and a complication rate of 17%. • Echocardiographically guided pericardiocentesis (often performed in the cardiac catheterization laboratory): This is usually performed from the left intercostal space. First, mark the site of entry based on the area of maximal fluid accumulation closest to the transducer. Then, measure the distance from the skin to the pericardial space. The angle of the transducer should be the trajectory of the needle during the procedure. Avoid the inferior rib margin while advancing the needle to prevent neurovascular injury. Leave a 16-gauge catheter in place for continuous drainage. • Percutaneous balloon pericardiotomy: This can be performed using an approach similar to that for echo-guided pericardiocentesis, in which the balloon is used to create a pericardial window
surgical • Surgical creation of a pericardial window: This involves the surgical opening of a communication between the pericardial space and the intrapleural space. This is usually a subxiphoidian approach with resection of xiphoid. Recently, a left paraxiphoidian approach with preservation of xiphoid has been described. Open thoracotomy and/or pericardiotomy3 may be required in some cases, and these should be performed by an experienced surgeon. • Pericardiocentesis or sclerosing the pericardium: This is a therapeutic option for patients with recurrent pericardial effusion or tamponade. Through the intrapericardial catheter, corticosteroids, tetracycline, or antineoplastic drugs (eg, anthracyclines, bleomycin) can be instilled into the pericardial space. • Pericardio-peritoneal shunt: In some patients with malignant pericardial effusions, creation of a pericardio-peritoneal shunt helps prevent recurrent tamponade. • Pericardiectomy: Resection of the pericardium (pericardiectomy) through a median sternotomy or left thoracotomy is rarely required to prevent recurrent pericardial effusion and tamponade.
Pathophysiology • The normal pericardium is composed of 2 layers: the tough fibrous parietal pericardium and the smooth visceral pericardium. Usually, approximately 50 mL of fluid (plasma ultrafiltrate) is present in the intrapericardial space to minimize friction during cardiac motion. • Acute and subacute forms of pericarditis (which may or may not be symptomatic) may deposit fibrin, which may, in turn, evoke a pericardial effusion. This often leads to pericardial organization, chronic fibrotic scarring, and calcification, most often involving the parietal pericardium
This thickened fibrotic pericardium, regardless of cause, impedes normal late diastolic filling, distinguishing constrictive from restrictive pericarditis. Since the myocardium is unaffected, early ventricular filling during the first third of diastole is unimpeded, but afterwards, the stiff pericardium affects flow and hemodynamics. In other words, the ventricular pressure decreases rapidly early (producing a steep y descent on right atrial pressure waveform tracings) and then increases abruptly to a level that is sustained until systole ("dip-and-plateau waveform" or "square root sign" seen on right or left ventricular pressure waveform tracings). • The clinical symptoms and classic hemodynamic findings can be explained by early rapid diastolic filling and elevation and equalization of the diastolic pressures in all of the cardiac chambers restricting late diastolic filling, leading to venous engorgement and decreased cardiac output, all secondary to a confining pericardium.
Physical findings • Constrictive pericarditis presents with a myriad of symptoms, making a diagnosis based solely on clinical history virtually impossible. Additionally, these symptoms may develop slowly over a number of years such that patients may not be aware of all of their symptoms until questioned. • Dyspnea tends to be the most common presenting symptom and occurs in virtually all patients. Fatigue and orthopnea are common. • Lower-extremity edema and abdominal swelling and discomfort are other common symptoms. Nausea, vomiting, and right upper quadrant pain, if present, are thought to be due to hepatic congestion, bowel congestion, or both. • The initial history may be more compatible with liver disease (cryptogenic cirrhosis) than with pericardial constriction because of the predominance of findings related to the venous system. • Chest pain, presumably due to active inflammation, may be present, although this is observed in a minority of patients.
muscle wasting, cachexia, or jaundice. • pleural effusion, hepatomegaly, or ascites. • Elevated jugular venous pressures • Sinus tachycardia • The apical impulse is often impalpable, and the patient may have distant or muffled heart sounds. • A pericardial knock, which corresponds with the sudden cessation of ventricular filling early in diastole, occurs in approximately half the cases and may be mistaken for an S3 gallop. However, a knock is of higher frequency than an S3 and occurs slightly earlier in diastole • The Kussmaul sign (ie, elevation of systemic venous pressures with inspiration) is a common nonspecific finding, but this sign is also observed in patients with right ventricular failure, restrictive cardiomyopathy, right ventricular infarction, and tricuspid stenosis, although, importantly, not in patients with cardiac tamponade.
Causes • Idiopathic • Infectious (tbc.bacterial . viral ) • Radiation-induced • Postsurgical • Neoplasms: • Uremia:. • Connective tissue disorders: • Drug-induced: Procainamide and hydralazine Methysergide therapy • Trauma:
Lab. • The level of brain natriuretic peptide (BNP), a cardiac hormone released in response to increased ventricular wall stretch, is often mildly increased in constrictive pericarditis (usually <150 ng/L). BNP levels are generally higher in restrictive cardiomyopathy (diagnostic if >650 ng/L) and may be useful in differentiating these disorders .
radiology Pericardial thickening of more than 4 mm assists in differentiating constrictive disease from restrictive cardiomyopathy, and a Thickening of more than 6 mm adds even more specificity for constriction
Echocardiography • an early diastolic septal notch or "septal bounce • evidence of right-sided pressure overload such as atrial septal shifting to the left with inspiration or dilated inferior and superior vena cavae and hepatic veins • Respiratory variation is usually greater in constriction than in restriction (probably because of the normal intraventricular septum), usually with over 25% changes. With restriction, often the E/A ratio is more than 2, the deceleration time is less than 150 ms, and the relaxation time is less than 60 ms. Unfortunately, when such Doppler findings are not present, the diagnostic reliability decreases. If a concomitant pericardial effusion is present, it may account for some respiratory variation . • Tissue Doppler echocardiography, measures the actual endocardial and epicardial tissue velocities. Since myocardial relaxation itself is preserved in pure constrictive pericarditis, the early relaxation myocardial velocity (Ea, also known as Em) is normal, whereas it is abnormal with restriction (when intrinsic myocardial disease is present). For example, given that a normal Ea is more than 10 cm/s, a near-normal (>8 cm/s) Ea supports constriction, whereas a much lower Ea supports restriction.16 The newer method of speckle tracking of B-mode images measures cardiac longitudinal and circumferential deformation. Patients with constrictive pericarditis were found to have constrained circumferential deformation rather than the longitudinal constraint found in patients with restrictive cardiomyopathy